We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Ultrasound: Abdomen
From WikEM
Contents
Background
- New techniques and findings on ultrasound of the abdomen can decrease time to diagnosis and patient/family satisfaction
- Ultrasound in not limited to FAST or aortic exams but can be used for appy’s, SBOs, and intussusception
Appendicitis
- Bedside ultrasound can be helpful in ruling in the diagnosis
- EDUS in adults has a Sn of 0.68 and Sp of 0.98[1]
- EDUS in pediatric has a Sn of 0.85 and Sp of 0.93[2]
Indications
- Classically symptoms include periumbilical pain traveling to the RLQ pain, followed by nausea, anorexia, and vomiting
Images
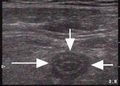
Instructions
- Use linear probe (curvilinear in more obese patients)
- Scan RLQ from ASIS to right iliac artery to identify a tubular structure
- Scanning over the point of maximal tenderness can be helpful
- The appendix typically appears anterior to the psoas muscle and iliac vessels
- Once identified, evaluate if the tube is compressible in the transverse view
Evaluation
- Accepted criteria for diagnosis includes[3]:
- Noncompressible
- Blind-ending tubular structure in the longitudinal axis
- Measures >6 mm in diameter from outer wall to outer wall
- Lacks peristalsis
- Other attributes can add to identification:
- Target-like appearance in the transverse axis
- Abdominal free fluid
- Wall edema
- Identification of fecalith
Small Bowel Obstruction
- EDUS had a Sn of 0.91 and Sp of 0.84 for SBO (compared to 0.02 and 0.67 respectively for Abd Xray)[4]
Indications
- Patients with crampy abdominal pain, paroxysms, and nausea/vomiting
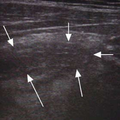
Images


Instructions
- Use curvilinear/phased array probe (linear probe can be used in very thin patients)
- Scan the entire abdomen using "lawn-mower" technique of horizontal tracks (or other systematic method)
- Scanning over dependent areas yields the most success
- Identify dilated loops of bowel
Evaluation
- SBO criteria include:
- Dilated loops of bowel >2.5cm
- Bidirectional peristalsis
- Additional findings include:
- "Keyboard" sign which are finger-like projections that represent plicae circulares
- Bowel wall edema
- Intraabdominal free fluid
- Sonographic transition point
Intussusception
- With minimal training, ED providers have a Sn of 0.85 and Sp 0.97[5]
Indications
- Classically a child from 3-36 mos with colicy pain, palpable mass on the right, and current jelly stool
Images
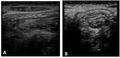

Instructions
- Use linear probe
- Scan from the cecum in the RLQ towards the RUQ
- Scanning over a palpable mass if felt can be helpful
- Identified the characteristic findings
Evaluation
- Longitudinal view shows a dilated intussuscipiens containing the intussusceptum
- This forms three parallel hypoechoic layers separated by hyperechoic zones
- Pseudokidney sign can be seen if mesentery is only on one side of the bowel
- Short axis shows a target sign of three parallel hypoechoic areas separated by hyperechoic zones
External Links
- Focus On: Ultrasound for Appendicitis
- Pediatric Ultrasound Tricks of the Trade: Abdominal Ultrasound
See Also
References
- ↑ Mallin M, et al. Diagnosis of appendicitis by bedside ultrasound in the ED. The American Journal of Emergency Medicine. 2014. 33(3):430 – 432.
- ↑ Sivitz A, et al. Evaluation of Acute Appendicitis by Pediatric Emergency Physician Sonography. Annals of Emergency Medicine. 2014. 64(4):358–364.
- ↑ Fox JC, et al. Prospective evaluation of emergency physician performed bedside ultrasound to detect acute appendicitis. Eur. J. Emerg. Med. 2008; 15(2):80-5.
- ↑ Jang TB, et al. Bedside ultrasonography for the detection of small bowel obstruction in the emergency department. J Emerg Med. 2011. 28(8):676-678.
- ↑ Riera A, et al. Diagnosis of intussusception by physician novice sonographers in the emergency department. Ann Emerg Med. 2012; 60(3):264–268.