Acute pain management
Contents
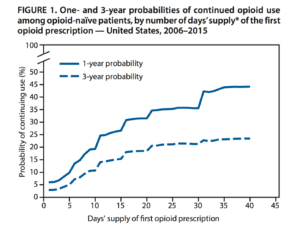
Opioid Epidemic
- Consider that with a 10-day supply of an initial opioid prescription, the odds of still being on opioids a year later is ~20%
- Consider opioid free regimens
WHO 3-step Ladder for Pain Control
| Agent | Oral | Parenteral |
|---|---|---|
| Step1. Mild Pain, Nonopioid, +/- Adjuvant | ||
| Acetaminophen | 650mg q4-q6h prn or 1000mg q6h prn | - |
| Aspirin | 650mg q4-6h prn or 1000mg q6h prn | - |
| Ibuprofen | 400-800mg q6-8h prn | - |
| Gabapentin (neuropathic Pain) | Start 300mg qhs | - |
| Step2. Mod Pain, Opioid for mild/mod pain, +/-nonopioid, +/-Adjuvant | ||
| Hydrocodone (5mg/Acetaminophen 325mg) | 1-2 tabs PO q4-6h prn | - |
| Oxycodone (5mg/Acetaminophen 325mg) | 1-2 tabs PO q4h prn | - |
| Oxycodone (Oxycontin) | 5mg q4-6h | - |
| Tramadol | 50-100mg q4-6h (max 400mg/day) | - |
| Step3. Severe Pain, Opioid for mod/sev pain, +/- nonopioid, +/-Adjuvant | ||
| Morphine | 10-30mg q3-4h | 0.1-0.2mg/kg(up to 15mg q4h) |
| Morphine (controlled release) | Start 30mg q8-12h , increase prn to 90-120mg q12h | - |
| Fentanyl | - | mcg/kg q1-3h |
| Hydromorphone (Dilaudid) | 2-4mg q4-6h | 1-4mg q4-6h |
| Levorphanol | 2mg q6-8h |
2mg q6-8h |
^In elders, use a bulk laxative and give instructions regarding activity, hydration and close follow-up
General Opioid Analgesics Chart
|
DRUG |
TYPICAL ADULT DOSE |
PHARMACOKINETICS |
COMMENTS |
|
0.1 mg/kg IV 10mg IM 0.3 mg/kg PO |
Onset: 1-2 min (IV), 10-15 min (IM/SC) Peak effect: 3-5 min (IV), 15-30 min (IM) Duration: 1-2 h (IV), 3-4 h (IM/SC) |
| |
|
(Dilaudid) |
0.015 mg/kg IV 1-2 mg IM |
Onset: 3-5 min (IV) Peak effect: 7-10 min (IV) Duration: 2-4 h (IV) |
|
|
1.0 mcg/kg IV |
Onset: <1 min (IV) Peak effect: 2-5 min (IV) Duration: 30-60 min (IV) |
| |
|
(Demerol) |
1.0-1.5 mg/kg IV/IM |
Onset: 5 min (IV) Peak effect: 5-10 min (IV) Duraction 2-3 h (IV) |
|
|
5-10 mg PO 30 mg PR |
Onset: 10-15 min (PO) Duration 3-6 h (PO) |
| |
|
5-10 mg PO |
Onset: 30-60 min (PO) Duraction 4-6 h (PO) |
| |
|
30-60 mg PO 30-100 mg IM |
Onset: 30-60 min (PO) Duraction: 4-6 h (PO) |
| |
|
(Ultram) |
50-100 mg PO |
Onset: 10-15 min (PO) Duration: 4-6 h (PO) |
|
Non-Opioid Analgesics Chart
| DRUG
|
TYPICAL ADULT DOSE
|
COMMENTS
|
| Acetaminophen |
650-1000mg PO q4h 1-2 g PO q4h |
|
| Aspirin | 650-1000mg PO q4h |
|
| Ibuprofen | 400-800mg PO q4-6h |
|
| Naproxen |
250mg PO q6-8h 500-1000mg PR q6-8h |
|
| Indomethacin |
25-50mg PO q12h 100mg PR q24h |
|
| Ketorolac |
15-30mg IV q6h 30-60mg IM |
|
Parenteral Opioid Dosing Chart
| DRUG | ROUTE | DOSAGE | COMMENTS |
| Morphine | IV or IM |
Titrate 2-5 mg increments q5-10 min Peak analgesia in 10-20 min Average: 10 mg q3-4h |
Preferred first-line agent in most situations |
| Fentanyl | IV or IM |
Titrate 25-50 mcg increments q2-3 min Peak analgesia in 3-5 min Duration 30-60 min |
Ideal for short procedures No histamine release Typically not suitable for the ED |
|
(Demerol) |
IV |
Titrate 12.5-50 mg increments Peak analgesia in 5-10 min Average: 100 mg q2-3h |
Risk of unique CNS toxicity with repeated dosing IM injection is very irritating to tissue |
|
(Dilaudid) |
IV |
Titrate 0.5-1.0 mg increments Peak analgesia in 5-15 min Average: 1.5 mg q3-4h |
|
|
(Stadol) |
IV |
Titrate 0.5-2.0 mg increments Peak analgesia in 4-5 min Average: 2 mg q3-4h |
Mixed agonist-antagonist May be preferred in biliary colic |
Oral Opioid Dosing Chart
| DRUG | ANALGESIC EQUIVALENCE | USUAL STARTING DOSE | USUAL INTERVAL |
| Morphine (MSIR, Roxanol, others) | 30 mg | 15-30 mg | 3-4 h |
| Morphine: sustained release (MS Contin, Oramorph-SR) | 30 mg | 30 mg | 8-12 h |
| Meperidine (Demerol) | 300 mg | 50-100 mg | 2-3 h |
| Codeine (in Tylenol #3, others) | 200 mg | 30-60 mg | 3-4 h |
| Oxycodone (Roxicodone, also in Percocet, Percodan, Tylox, others) | 20-30 mg | 5-10 mg | 3-6 h |
| Hydrocodone (in Lorcet, Lortab, Vicodin, others) | 30 mg | 5-10 mg | 3-6 h |
| Hydromorphone (Dilaudid) | 7.5 mg | 4-8 mg | 2-3 h |
| Tramadol (Ultram) | N/A | 25-50 mg | 4-6 h |
See Also
- Opioid overdose
- Opioid withdrawal
- Analgesics and Sedatives (Pediatrics)
- Complex regional pain syndrome
References
Adapted from Tintinalli and Harwood & Nuss, World Health Organization 3-Step Analgesia Ladder for Cancer & Washington Manual Intership Survival Guide, 2008