We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Open-angle glaucoma
From WikEM
Contents
Background
- An optic neuropathy characterized by an increase in intraocular pressure leading to damage to the optic nerve and irreversible vision loss.
- Second leading cause of irreversible blindness worldwide
Risk Factors
- Age (4% prevalence in age >80)
- Race (3 times higher in Black patients)
- Family History (2-3 fold increase for individuals with affected sibling or parent)
- Hypertension
- Diabetes
- Other: Myopia, pseudoexfoliation, low diastolic perfusion pressure, cardiovascular disease, hypothyroidism
Pathophysiology
Not entirely clear, but may be related to an increased intraocular pressure that leads to compression of the optic nerve at the site where it exits the eye. This causes a progressive decrease in the number of retinal ganglion cells.
Clinical Features
Most commonly presents with progressive peripheral vision loss, followed by central vision loss
- Painless
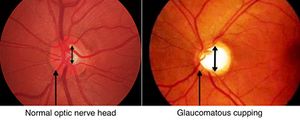
- Cupping of the optic disc
- Loss of peripheral visual field
- Preservation of central vision
Differential Diagnosis
Acute Vision Loss (Noninflamed)
- Arteritic anterior ischemic optic neuropathy
- Amaurosis fugax
- Central retinal artery occlusion (CRAO)†
- Central retinal vein occlusion (CRVO)†
- High altitude retinopathy
- Open-angle glaucoma
- Optic neuritis
- Posterior Reversible Encephalopathy Syndrome (PRES)
- Retinal detachment†
- Temporal arteritis†
- Traumatic optic neuropathy
- Vitreous hemorrhage
- Stroke†
†Emergent Diagnosis
Evaluation
Testing
Fundus examination
- Cupping >50% of the vertical disc diameter
- Thinning or notching of disc rim
- Progressive change of size/shape of cup
Visual field testing
Intraocular pressure
- Does not establish diagnosis of Open angle glaucoma. 1/2 of patients with OAG have normal intraocular pressure
- Normal Intraocular pressure ranges from 10 to 20 mmHg
- Pressure >21 mmhg considered ocular hypertension
Diagnosis
At least one of the following:
- Evidence of optic nerve damage from structural abnormalities (thinning, cupping, notching of disc rim)
- Adult Onset
- Open, normal appearing anterior chamber angles
- Absence of known secondary causes of open-angle glaucoma
Management
- β-blockers: Timolol maleate 0.25%-0.5%, one drop BID
- α-adrenergic agonist: Brimonidine 0.2% one drop BID
- Carbonic Anhydrase inhibitors: Dorzolamide 2% one drop BID
- Prostaglandins: Latanoprost 0.005% one drop qD
- Persistent elevated intraocular pressures: Acetazolamide 125-250mg PO bid-qid
Disposition
Indications for ophthalmologic referral:
- IOP>40mmHg: emergency referral
- IOP 30-40 mmHg: referral within 24hr if no symptoms suggesting acute glaucoma
- IOP 25-29 mmHg: Evaluation within 1 week
- IOP 23-24 mmHg: repeat measurement and referral for comprehensive eye examination
See Also
External Links
References
- Tsai LM, Pitha I, Kamenetzky SA. The Eye & Ocular Adnexa. In: Doherty GM. eds. CURRENT Diagnosis & Treatment: Surgery, 14e. New York, NY: McGraw-Hill; 2015.
- Weinreb RN, Khaw PT. Primary open-angle glaucoma. Lancet 2004; 363:1711
- UpToDate
- American Academy of Ophthalmology, Glaucoma Panel. Primary open-angle glaucoma. Preferred practice pattern. San Francisco: American Academy of Ophthalmology, 2000:1–36