IVC ultrasound
Contents
Background
- Though controversial, IVC measurement by ultrasound can estimate volume status, fluid responsiveness, and fluid tolerance
- Can use as a dynamic assessment after intervention such as giving fluids or passive leg raise
- Dynamic changes is probably best measured in intubated patients
Indications
- Differentiate causes of shock
- Differentiate causes of shortness of breath
Technique
- Select probe
- Curvilinear or phased array probe
- Location
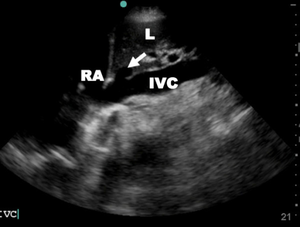
- In subxyphoid cardiac view (epigastric), fan probe laterally to view the IVC draining and identify it draining into the right atrium
- May start with subxyphoid view, place right atrium in center of screen and rotate probe 90 degrees clockwise to find IVC
- Longitudinal view
- M-mode to measure IVC collapse during inspiration or estimation can be made in 2D with IVC in longitudinal axis
- Measure both absolute diameter of IVC and percent collapse during inspiration of spontaneously breathing patients
- Dynamic measurements
- Repeat measurements can be made after passive leg raise or IVF bolus
Findings
Classic Ultrasound Findings For Critically Ill Patients
| Disease | IVC | Cardiac | Lung (Phased Array) | Lung (Linear) |
|---|---|---|---|---|
| MI | ↑ | Focal WMA Mod/Poor squeeze |
NL or B-lines | Sliding |
| Tamponade | ↑ | RA collapse with filling RV collapse with filling |
NL | Sliding |
| PTX | ↑ | NL or Hyperdynamic | Lung point Consolidated lung |
Absent lung sliding |
| Sepsis | ↓ | Hyperdynamic squeeze | NL (see pneumonia) | Sliding |
| Pneumonia | NL or ↓ | Hyperdynamic squeeze | Unilateral B-lines | Sliding |
| Decompensated HF | ↑ | Mod/Poor squeeze | Bilateral B-lines | Sliding |
| PE | ↑ | RV > LV McConnell's sign |
NL or Unilateral B-lines | Sliding |
Correlations Between IVC Size and CVP[3]
| IVC (cm) | Respiratory Change | CVP (cm H2O) |
|---|---|---|
| <1.5 | Total collapse | 0-5 |
| 1.5-2.5 | >50% collapse | 6-10 |
| 1.5-2.5 | <50% collapse | 11-15 |
| >2.5 | <50% collapse | 16-20 |
| >2.5 | No change | >20 |
Measure 2cm from IVC/RA junction or 1cm from IVC/hepatic vein junction
Images
Pearls and Pitfalls
- Aorta can be confused for IVC, ensure your visualize the vessel entering the atrium
- Ensure the vessel is viewed in full longitudinal axis as being off center will give falsely narrow measurements
Documentation
Normal Exam
A bedside IVC ultrasound was performed to assess volume status in setting of dehydration. The IVC was identified in longitudinal access. The IVC was neither flat nor plethoric. There was less than 50% collapse with respirophasic measurements. This does not imply that the patient is not volume responsive but rather further testing is needed.
Abnormal Exam
A bedside IVC ultrasound was performed to assess volume status in setting of dehydration. The IVC was identified in longitudinal access. The IVC was flat with over 50% collapse with respirophasic measurements. There was evidence of volume depletion and fluid tolerance.
A bedside IVC ultrasound was performed to assess volume status in setting of fluid overload. The IVC was identified in longitudinal access. The IVC was plethoric with less than 50% collapse with respirophasic measurements. There was evidence of volume overload.
Clips
Normal IVC


Flat IVC


Plethoric IVC


Video
External Links
- Life in the Fastlane - SMACC: The Dark Art of IVC Ultrasound
- ACEP Focus On: Inferior Vena Cava Ultrasound
See Also
References
- ↑ Dipti A, et al. Role of inferior vena cava diameter in assessment of volume status: a meta-analysis. AJEM. 2012; 30:1414-1419.
- ↑ Zhang Z, et al. Ultrasonographic measurement of the respiratory variation in the inferior vena cava diameter is predictive of fluid responsiveness in critically ill patients: systematic review and meta-analysis. Ultrasound Med Biol. 2014. May; 40(5):845-53.
- ↑ Goldflam K, et al. Focus on: Inferior vena cava ultrasound. ACEP News. June 2011.