We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Hyperosmolar hyperglycemic state
From WikEM
(Redirected from Hyperosmolar coma)
Contents
Background
- Prototypical patient is elderly with uncontrolled type II DM without adequate access to H2O
- Occurs due to 3 factors:
- Insulin resistance or deficiency
- Increased hepatic gluconeogenesis and glycogenolysis
- Osmotic diuresis and dehydration followed by impaired renal excretion of glucose
- May result in TBW losses of 8-12L
- Ketosis usually absent (may be mild)
- Cerebral edema is uncommon complication (case reports)
Precipitants
- Pneumonia (Main)
- Urinary tract infection
- Medication non-adherence
- Cocaine intoxication
- Meds: Beta-blockers, diuretics
- GI bleed
- Pancreatitis
- Heat related emergencies
- Acute coronary syndrome
- Stroke
Clinical Features
- Dehydration
- Seizure (15% of patients)
- Altered mental status
- Lethargy/coma
Differential Diagnosis
Hyperglycemia
- Diabetic foot infection
- Diabetic ketoacidosis (DKA)
- Diabetic ketoacidosis (peds)
- Hemochromatosis
- Hyperosmolar hyperglycemic state (HONC)
- Iron toxicity
- New onset diabetes mellitus
- Nonketotic hyperglycemia
- Sepsis
Evaluation
Work Up
- Chem
- Serum Osm
- Lactate
- Serum ketones
- CBC
- Also consider:
- Blood cultures
- Urinalysis/Urine culture
- LFTs
- Lipase
- Troponin
- CXR
- ECG
- Head CT
Evaluation
- Glucose >600
- Osm >315
- Bicarb >15
- pH >7.3
- Serum ketones negative or mildly positive
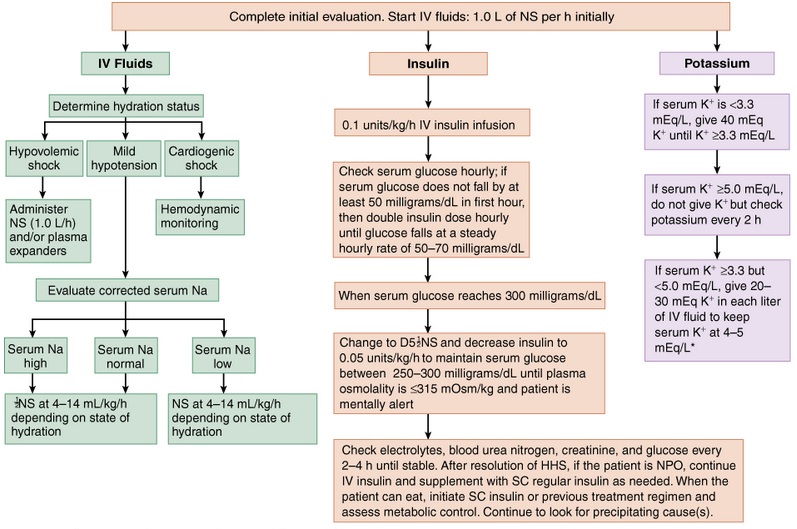
Management
- Fluid replacement
- Average fluid deficit is 8-12L
- 50% should be replaced over the initial 12hr
- May have to replace slower if patient has cardiac/renal impairment
- Aggressiveness of fluid replacement must be weighed against the risk of cerebral edema, which increases with younger age[1]
- Average fluid deficit is 8-12L
- Hypokalemia
- Must treat aggressively
- Once adequate urinary output has been established K+ replacement should begin
- Hyperglycemia
- Do not start insulin until K > 3.3 and adequate urinary output has been established
- Hypomagnesemia
- Repletion will help correct hypokalemia
- Hypophosphatemia
- Routine correction unnecessary unless phos <1.0
Disposition
- Most patients require ICU admission
See Also
References
- ↑ Stoner GD. Hyperosmolar Hyperglycemic State. Am Fam Physician. 2005 May 1;71(9):1723-1730. http://www.aafp.org/afp/2005/0501/p1723.html