We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Pleural effusion
From WikEM
(Redirected from Hydrothorax)
Contents
Background
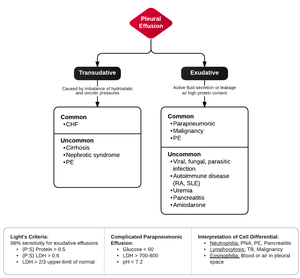
- Exudative
- Active fluid secretion or leakage with high protein content
- Transudative
- Imbalance between hydrostatic (e.g. CHF) and oncotic (e.g. nephrotic syndrome)
- Fluid has low protein content
Evaluation
Detection
- CXR
- Earliest sign is blunting of costophrenic angle
- PA view requires 200-250cc of fluid; Lateral requires 50-75cc of fluid
- Supine view may only show a generalized hazy appearance of affected hemithorax
- Subpulmonic effusion
- Fluid collects in isolation between lung base and diaphragm
- May not cause blunting of costophrnic angle or meniscus appearance
- Suspect if "hemidiaphragm" (actually fluid) is elevated and flattened
- Lateral decubitus with suspected side down will show free-flowing pleural fluid
- CT
- US
Exudative versus Transudative (Light's Criteria)
- If one of the following is present the fluid is virtually always an exudate
- If none is present the fluid is virtually always a transudate
- Pleural fluid/serum protein ratio >0.5
- Pleural fluid/serum LDH ratio >0.6
- Pleural fluid LDH > two thirds of upper limit for serum LDH
Exudative Work-up
- Gram stain and culture (place 10cc into blood culture bottle at the bedside)
- Cell count
- RBC >100K: trauma, malignancy, pneumonia, or pulmonary infarction
- Neutrophil predominance (>50%): parapneumonic, pulmonary embolism, pancreatitis
- Lymphocytic predominance (>50%): malignancy, TB, PE, viral pleuritis
- Glucose
- Low glucose (<60) seen in parapneumonic, empyema, malignant, TB, and RA
- ABG (pH)
- May be left at room temperature for up to 1hr with out affecting results
- Normal pleural fluid pH = 7.64;
- In parapneumonic effusions, <7.10 predicts development of empyema or persistence and indicates need for thoracostomy tube drainage
- Amylase: >100 in pleural effusions due to pancreatitis or esophageal rupture
- TB (adenosine deaminase)
- India ink
- Cytology (requires 50cc)
Work-Up
Differential Diagnosis
Common
- Transudative
- Exudative
Less Common
- Transudative
- Nephrotic Syndrome
- Cirrhosis
- Both via hypoalbuminemia and transdiaphragmatic leakage of ascites
- PE
- Exudative
- Viral, fungal, or parasitic infection
- SLE, RA
- Uremia
- Pancreatitis
- Amiodarone
Non-infectious Effusions
- Left sided > R
- Right sided > L
Management
- Dyspnea at rest
- Therapeutic thoracentesis with max drainage 1-1.5L to avoid reexpansion pulmonary edema
- Patient positioning (lateral decubitus) for unilateral pleural effusions
- Most of the time, "Good lung to Ground" to improve V/Q mismatch
- Exceptions in which "bad" lung should be "down":
- Massive hemoptysis
- Severe/large pleural effusions
- Large pulmonary abscesses
- Empyema
- Drain with large-bore thoracostomy tube
- Parapneumonic Effusion
- Consider thoracostomy tube drainage if:
- Comorbid disease
- Failure to respond to antibiotic treatment
- Anaerobic organisms
- Pleural fluid pH <7.10
- Effusion involving >50% of thorax or air-fluid level on CXR
- Loculated effusion
- Consider thoracostomy tube drainage if:
- CHF
- Diuretic therapy resolves >75% of effusions within 2-3d
See Also