We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Angioedema
From WikEM
(Redirected from Hereditary angioedema)
Contents
Background
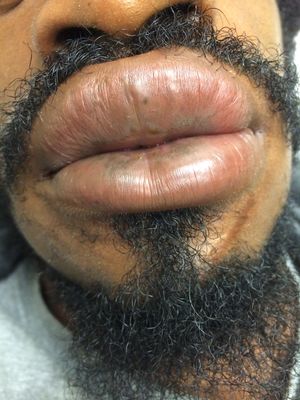
- Angioedema is paroxysmal, nondemarcated swelling of dermal or submucosal layers of skin or mucosa
- Swelling is asymmetric, nonpitting, and nonpruritic, however can be associated with allergic features depending on cause
Etiologies
- Allergic angioedema: IgE–mediated type I hypersensitivity reaction
- Hereditary angioedema: Congenital or acquired loss of C1 esterase inhibitor
- ACE-Iinduced angioedema: ACEI adverse reaction from excessive bradykinin
- Idiopathic angioedema

Hereditary angioedema
Background
- Due to C1 esterase inhibitor deficiency
- Leads to unregulated activity of vasoactive mediators (bradykinin) associated with complement pathway
- Autosomal dominant
- Edema of face, extremities, bowel wall
Evaluation
- Suspect in patients with history of recurrent peripheral angioedema and abdominal pain
- 75% experience onset of symptoms before age 15yr
- C4 level screens for HAE (suspect if low)
- Decreased levels of C1 and C4 esterase inhibitors confirms diagnosis
ACE inhibitor-induced angioedema
Background
- Incidence is highest within the first month; however, may occur at anytime
- 40% present months to years after initial dose[1]
- Incidence is 0.1-2.2% (more common in blacks)
- Physiology more closely related to bradykinin-mediated pathway than IgE-mediated pathway, therefore current treatments may be insufficient
Differential Diagnosis
Acute allergic reaction
- Allergic reaction/urticaria
- Anaphylaxis
- Angioedema
- Asthma exacerbation
- Anxiety attack
- Scombroid
- Cold urticaria
- Contrast induced allergic reaction
- Shock
- Transfusion reaction
- Carcinoid syndrome
Management
General
- Consider Epinephrine 0.3mg IM if there is any concern this could be allergic in nature
- Consider Glucagon 1-5mg IV if patient is on beta-blockers and not responding to Epinephrine
- FFP for possible etiology related to bradykinin[2]
- 2 units
- Consider definitive airway if voice change, hoarseness, stridor, dyspnea
- Prepare for a difficult airway which can include need for fiberoptics, ENT/anesthesia assistance, surgical airway, or transfer to the OR
Hereditary Angioedema
First-Line Therapies
- C1 inhibitor (C1INH)[3]
- 1000 units if ≤50kg
- 1500 units if >50-75kg
- 2000 units if >75-100kg
- 2500 units if >100kg
- Ecallantide
- 10mg SQ x 3 in different anatomical locations (30mg in total)
- Icatibant
- 30mg SQ
ACE-I Induced Angioedema
- Typical anaphylaxis medications do not effect bradykinin levels[4], but consider:
- Epinephrine 0.3mg IM
- Diphenhydramine 50mg IV
- Methylprednisolone 125mg IV
- Icatibant
- 30mg SQ
- Significantly decreases time to complete resolution (8 hrs vs 27.1 hrs)[5]
- Note: control group did not receive FFP
- Consider Ecallantide
Disposition
- Consider discharge after 4-6 hrs observation if there is no airway edema and patient improves
- 24 hrs obs if epinephrine given
- Ishoo Staging (based on retrospective study)[8]
- Stage 1 - face/lip
- 48% outpatient, 52% floor, 0% ICU or advanced airway
- Stage 2 - soft palate
- 60% outpatient, 40% floor, 0 ICU or advanced airway
- Stage 3 - tongue
- 26% outpatient, 67% ICU, 7% advanced airway
- Stage 4 - larynx
- 100% ICU, 24% advanced airway
- Stage 1 - face/lip
See Also
References
- ↑ Winters ME, et al. Emergency department management of patients with ACE-inhibitor angioedema. JEM. 2013; 45(5):775–780.
- ↑ Moellman, J.J., Bernstein, J.A., Lindsell, C., Banerji, A., Busse, P.J., Camargo, C.A., Collins, S.P., Craig, T.J., Lumry, W.R., Nowak, R., Pines, J.M., Raja, A.S., Riedl, M., Ward, M.J., Zuraw, B.L., Diercks, D., Hiestand, B., Campbell, R.L., Schneider, S. and Sinert, R. (2014) ‘A consensus parameter for the evaluation and management of Angioedema in the emergency department’, Academic Emergency Medicine, 21(4), pp. 469–484.
- ↑ Craig TJ, Levy RJ, Wasserman RL, et al. Efficacy of human C1 esterase inhibitor concentrate compared with placebo in acute hereditary angioedema attacks. J Allergy Clin Immunol. 2009; 124(4):801.
- ↑ Bas M, Greve J, Stelter K, et al. Therapeutic efficacy of icatibant in angioedema induced by angiotensin-converting enzyme inhibitors: a case series. Ann Emerg Med. 2010; 56(3):278-282.
- ↑ Baş M, Greve J, Stelter K, et al. A randomized trial of icatibant in ACE-inhibitor-induced angioedema. N Engl J Med. 2015; 372(5):418-25.
- ↑ Bernstein JA, Moellman JJ, Collins SP, et al. Effectiveness of ecallantide in treating angiotensin-converting enzyme inhibitor-induced angioedema in the emergency department. Ann Allergy Asthma Immunol. 2015; 114(3):245.
- ↑ Lewis, L.M., Graffeo, C., Crosley, P., Klausner, H.A., Clark, C.L., Frank, A., Miner, J., Iarrobino, R. and Chyung, Y. (2015) ‘Ecallantide for the acute treatment of angiotensin-converting enzyme Inhibitor–Induced Angioedema: A Multicenter, Randomized, controlled trial’, Annals of Emergency Medicine, 65(2), pp. 204–213.
- ↑ Ishoo E, et al. Predicting airway risk in angioedema: staging system based on presentation. Otolaryngol Head Neck Surg. 1999; 121(3):263-268.