We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
External hemorrhoid
From WikEM
Contents
Background
- Pathologic state cccurs when internal or external hemorrhoid plexus become engorged, prolapsed, or thrombosed
- Bleeding is usually limited (surface of stool, on toilet tissue, at end of defecation)
- Passage of blood clots requires evaluation for colon lesions
Risk Factors
- Constipation and straining at stool
- Frequent diarrhea
- Older age
- IBD
Clinical Features


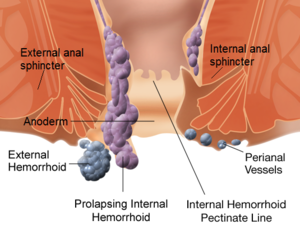
- Occur distal to dentate line
- Can be seen at external inspection
- More prominent with Valsalva
- Thrombosed hemorrhoids (bluish-purple discoloration) cause painful defecation
- Non-thrombosed hemorrhoids are usually painless
- If patient complains of pain but hemorrhoids are not thrombosed suspect:
- Perianal/intersphincteric abscesses
- Anal fissures
- If patient complains of pain but hemorrhoids are not thrombosed suspect:
- Non-thrombosed hemorrhoids are usually painless
- Prolapse
- Requires periodic reduction by the patient
Differential Diagnosis
Anorectal Disorders
- Anal tags
- Hemorrhoids
- Internal hemorrhoid
- External hemorrhoid
- Cryptitis
- Anal fissure
- Anal fistula
- Anorectal abscess
- Proctitis
- Rectal prolapse
- Rectal foreign body
- Pruritus ani
- Pilonidal cyst
- Constipation
- Condyloma acuminata
- Anal cancer
- Colorectal tumor
- Pedunculated polyp
- Crohn Disease
- Syphilitic fissure
- GC/Chlamydia
Lower gastrointestinal bleeding
- Upper GI Bleeding
- Diverticular disease
- Vascular ectasia
- Inflammatory bowel disease
- Infectious colitis
- Mesenteric Ischemia
- Meckel's diverticulum
- Malignancy / polyps
- Hemorrhoids
- Internal hemorrhoid
- External hemorrhoid
- Aortoenteric fisulta
- Rectal foreign body
- Rectal ulcer (HIV, Syphilis, STI)
- Anal fissure
Management
Not Thrombosed
- Usually self-limiting with resolution in 1 week
Thrombosed
- Consider sitz baths and bulk laxatives if:
- Thrombosis has been present >48 hr
- Swelling has started to shrink
- Pain is tolerable
- Conservative management with topical 0.3% nifedipine and 1.5% viscous lidocaine is alternative[1]
- Consider Perianal block for pain relief
- Consider excision if:
- Patient is not immunocompromised, child, pregnant woman, has portal hypertension, coagulopathic
- Thrombosis is acute (<48 hr)
- Extremely painful
- See External Hemorrhoid Excision
Disposition
See Also
External Links
References
- ↑ Perrotti P. Conservative treatment of acute thrombosed external hemorrhoids with topical nifedipine. Dis Colon Rectum. 2001 Mar;44(3):405-9.
Authors
Ross Donaldson, Kevin Lu, Devin Smith, Neil Young, Michael Holtz