We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Compartment pressure measurement
From WikEM
Contents
Indications
Compartment Syndrome Indications
- Consider whenever pain or paresthesia occurs in an extremity after:
- fracture
- crush injury
- immobilizaition
- snake bites
- burns
- prolongued tourniquet application
- fluid extravasation into a limb
- soft tissue infection
- extreme exertion
- Immediate threat is viability of nerve and muscle; later threat is infection, gangrene, Rhabdomyolysis, Renal Failure
Contraindications
- Avoid areas of cellulitis.
- No absolute contraindications
Equipment Needed
- All cases
- Chloroprep or other skin prep solution
- Lidocaine 1% without epi
- 5cc syringe
- 22g or 25g needle with enough length to reach compartment
- Stryker available
- Stryker Intra-Compartmental Pressure Monitor
- Prefilled syringe with saline
- Arterial line transducer
- Intracompartment needle (simple 18-gauge needle or 18-gauge spinal needle)
- High-pressure tubing
- Pressure transducer with cable
- Pressure monitor/module
- 1L NS with pressure bag
- Two 3-way stopcocks
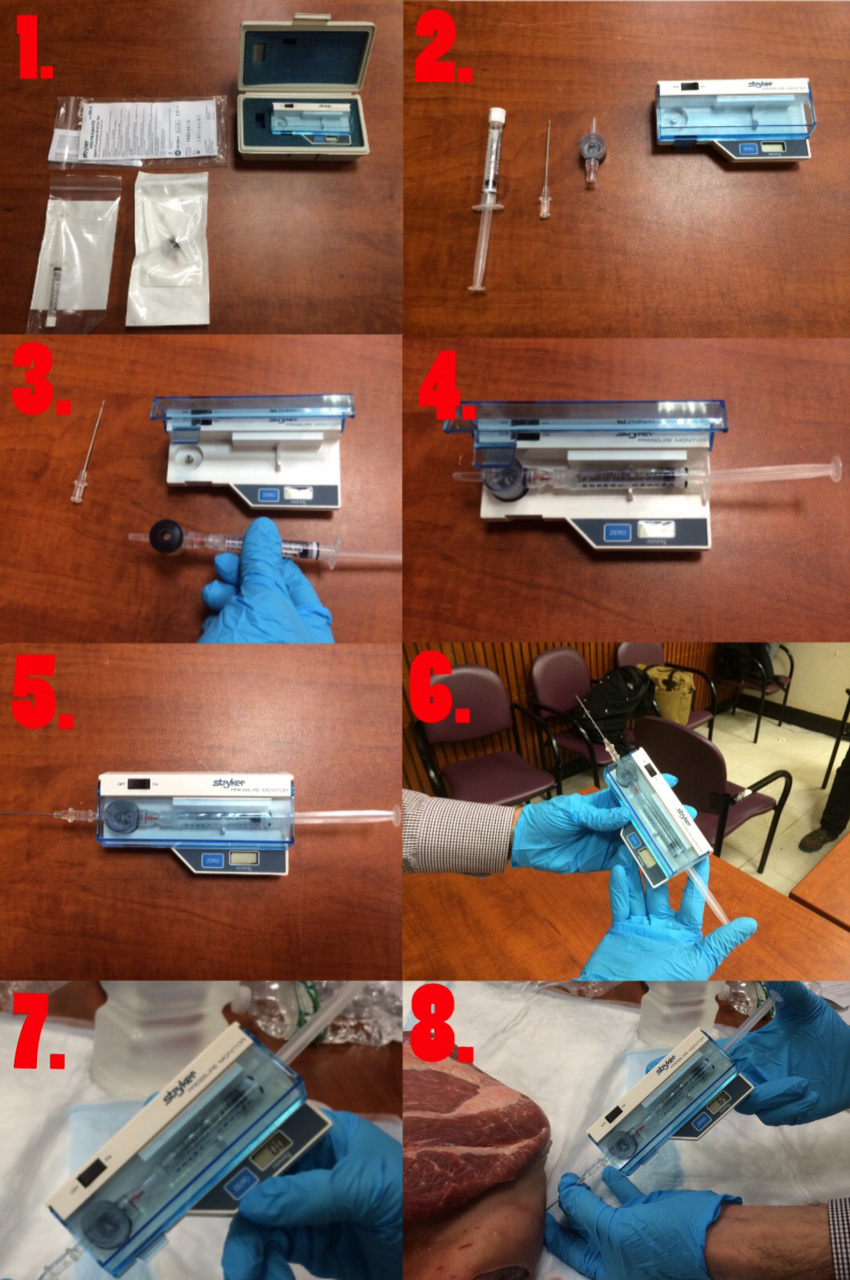
Procedure
- Contents of the pressure measurement kit
- Remove contents from wrapping
- Attach chamber to the pre-filled saline syringe
- Place the aforementioned into the monitor/unit
- Place needle onto chamber
- Eject excess air, if present, from syringe
- Zero the assembled unit at the angle you will be entering compartment
- Determine the appropriate site of injection to measure the desired compartment pressure
- Clean the area with alcohol prep or chlorhexidine.
- Insert, inject 2-3 drops of saline, and await measurement
Technique
- should be performed within 5cm of fracture site
- anterior compartment
- entry point: 1 cm lateral to anterior border of tibia
- needle should be perpendicular to skin
- deep posterior compartment
- entry point: just posterior to the medial border of tibia
- advance needle perpendicular to skin towards fibula
- lateral compartment
- entry point: just anterior to the posterior border of fibula
- superficial posterior
- entry point: middle of calf
Pressure Interpretation
- Normal is <10 mm Hg
- Pressures <20 mmHg can be tolerated w/o significant damage
- Exact level of pressure elevation that causes cell death is unclear. It was previously thought pressure >30 mmHg was toxic although the "delta pressure" may be better predictor than absolute pressure
ΔPressure = [Diastolic Pressure] – [Compartment Pressure][1]
- ΔPressure < 30 mm Hg is suggestive of compartment syndrome
Complications
- Infection
- Low risk
- Minimized by strict sterile technique
- Pain
- Minimized by local lidocaine infiltration
See Also
External Links
References
- ↑ Elliott, KGB. Diagnosing acute compartment syndrome. J Bone Joint Surg Br. 2003 Jul;85(5):625-32. PDF