We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Balloon tamponade
From WikEM
Contents
Indications
- Unstable patients with massive upper GI bleed and
- Inability to perform endoscopy
- Endoscopy failure
- Delay in consultant presentation
- Need to transfer/stabilize
Contraindications
- History of esophageal stricture
- Recent esophageal or gastric surgery
Equipment Needed
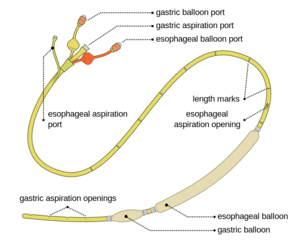
- Balloon device
- Sengstaken-Blakemore Tube
- Minnesota Tube
- 60 cc syringe
- Padded(tape) kelly clamps
- Used to clamp gastric and esophageal balloon ports to maintain precise pressure/volume
- Manometer
- 3-way connector device
- NG tube (only for Sengstaken-Blakemore)
- Kerlex
- IV pole
- 1 L bag IVF
Procedure
- Patient should be intubated prior to placement to decrease aspiration risk
- Test tubes for leaks and inflate in 100 mL increments while measuring the pressure each time
- If using Sengstaken-Blakemore tube, secure NG tube to tamponade device with distal end of NG tube 3 cm proximal to esophageal balloon
- This will function as esophageal aspiration port
- Insert tube orally to at least 50 cm mark
- Use lubrication and laryngoscope to aid in placement
- Inject air into gastric port and listen over the stomach
- If air is auscultated, inject 50 cc into gastric balloon and shoot CXR to confirm placement in stomach
- Gastric aspiration port to continuous suction
- Completely fill gastric balloon
- Sengstaken-Blakemore: 250-300cc
- Minnesota: 450-500cc
- Measure the pressure at each 100 mL increment
- If pressure is >15mm Hg more than corresponding pre-insertion pressure deflate the balloon and advance further prior to filling gastric balloon
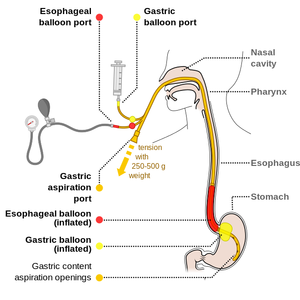
- Place 1 kg traction on tamponade device and mark device at the lips
- Tie one end of kerlex around the distal portion of tamponade device (proximal to port insertion sites) and attach other end to 1 L bag IVF
- Hang 1 L bag over IV pole
- Esophageal and gastric aspiration ports to suction
- If bleeding continues inflate the esophageal balloon
- Inflate to 20-40 mm Hg
- Do not inflate more than 45 mm Hg
Complications
- Due to misplaced balloon, migration, overinflation, prolonged use
- Mucosal ulceration
- Aspiration
- Airway or large vessel obstruction
- Esophageal rupture
See Also
External Links
- LITFL: Sengstaken-Blackmore and Minnesota Tubes
- EMCRIT: Blakemore Tube Placement for Massive Upper GI Hemorrhage
Sources
- Roberts & Hedges 41, pp 831-836