We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Aortic stenosis
From WikEM
(Redirected from Aortic Stenosis)
Contents
Background
- Younger patients: usually from a congenital bicuspid valve
- Older patients: usually from calcifications on aortic valve
- Rhumatic heart disease is the next most common
- Significant obstruction when orifice <1 cm or pressure grad is >50 mmHg
Clinical Features
- Dyspnea, chest pain, syncope
- Once symptoms present mean survival is 2-3yr
- Ejection systolic murmur radiating to carotids
- Pulsus parvus et tardus - slow to rise and late peaking
- Narrowed pulse pressure
- Soft 2nd heart sound
Differential Diagnosis
Valvular Emergencies
- Mitral stenosis
- Mitral regurgitation
- Aortic stenosis
- Aortic regurgitation
Evaluation
- Echocardiography, TTE findings
- Minimal excursion of the aortic valve leaflet
- Calcifications of AV
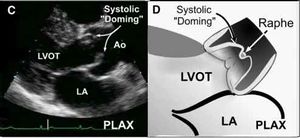
- Systolic "doming" on parasternal long
- Turbulent flow through AV on color doppler
- LV hypertrophy
- Number of leaflets (unicuspid, bicuspid, tricuspid, quadricuspid)[1]
- Raphe in bicuspid aortic valve in diastole may false negatively appear like trileaflet valve
- Only comment on the number of leaflets in systole in parasternal short axis
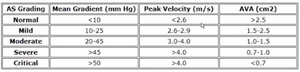
- Severity by continuous wave (CW) Doppler peak velocity (m/s)[2]
- AS is unlikely if peak CW velocity well below 2.5 m/s, and AVA measurements may not be necessary
- Ensure parallel intercept angle across aortic valve in apical view
- < 2.5 = aortic sclerosis
- 2.6 - 2.9 = mild
- 3.0 - 4.0 = moderate
- > 4.0 = severe
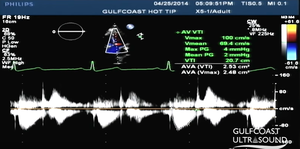
- Aortic valve area (AVA) requires LVOT diameter (D) and velocity time integral (VTI) at LVOT and AV in the continuity equation
- More reliable than CW doppler peak velocity
- Obtain LVOT diameter just apical to AV in PSL at maximal systole
- Obtain the following in apical view at the aortic valve as parallel to flow as possible to avoid falsely low values
- AV VTI (continuous wave doppler), gate at tips of AV opening in systole, tracing below the line in systole
- LVOT VTI (pulse wave doppler), gate in LVOT just apical to AV, tracing below the line in systole
- Aortic stenosis valve area severity[3]
- Normal, > 2.5 cm²
- Mild, 2.5 - 1.5 cm²
- Moderate, 1.0 - 1.5 cm²
- Severe, < 1.0 cm²



- Caveats in TTE for AS
- Eccentric mitral regurgitation jets may interfere with AV flows
- Atrial fibrillation poses different levels of diastolic and systolic filling, requiring multiple tracings
- Poor LV function may reduce velocities upon measuring, while AS may still be present
Management
- Avoid negative inotropes such as beta-blockers, calcium-channel blockers
- Afterload reduction is controversial and in decompensated AS should only be conducted in a monitored setting
- Consider cardiology consult
- AS + A-fib = emergency
- Consider emergent cardioversion
- Pulmonary edema
- Diuretics, NIV, and intubation if necessary
- Extreme caution with use of nitrates/vasodilators (preload reducers)
- In critical cases, particularly in those unstable to undergo emergent surgery, balloon aortic valvuloplasty may be an option as bridge to AVR or palliative care in nonsurgical candidates
Disposition
- Severe HF symptoms resistant to medical management require urgent surgery
- Class I indications for AVR:
- Severe AS in symptomatic pt
- Severe AS undergoing CABG, aortic, or valve surgery
- Severe AS with LV dysfunction, EF < 50%
See Also
- Valvular emergencies
- Heart murmurs
- Cardiogenic shock
- See Intro to Aortic Stenosis by Joseph Minardi on YouTube
References
- ↑ Baumgartner H et al. Echocardiographic assessment of valve stenosis: EAE/ASE recommendations for clinical practice. European Journal of Echocardiography (2009) 10, 1–25.
- ↑ Baumgartner H, Hung J, Bermejo J, Chambers JB, Evangelista A, Griffin BP, Iung B, Otto CM, Pellikka PA, Quiñones M, American Society of Echocardiography, and European Association of Echocardiography. Echocardiographic assessment of valve stenosis: EAE/ASE recommendations for clinical practice. J Am Soc Echocardiogr. 2009 Jan;22(1):1-23; quiz 101-2.
- ↑ Saito T et al. Prognostic value of aortic valve area index in asymptomatic patients with severe aortic stenosis. Am J Cardiol. 2012 Jul 1;110(1):93-7.