We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Ankle fracture
From WikEM
Contents
Background
Clinical Features
- Examine for ecchymoses, abrasions, or swelling
- vascular and neurologic assessment
- DPs and PTs
- 4 sensation distributions: saphenous nerve (medial mal), superficial fib (lat mal), sural nerve (lateral 5th digit), deep fib (1st web space)
- Note skin integrity and areas of tenderness or crepitus over ankle
- Range joint passively and actively to evaluate for stability
- Examine Joints above and below the ankle
- Perform anterior drawer test (positive exam suggests torn ATFL)
- Always palpate entire length of fibula to rule-out Maisonneuve Fracture (fibulotibialis ligament tear)
- Perform a crossed-leg test to detect syndesmotic injury
- Evaluate integrity of Achilles tendon (Thompson test)
- Palpate midfoot and base of 5th metatarsal for tenderness
Differential Diagnosis
Other Ankle Injuries
Distal Leg Fractures
- Tibial plateau fracture
- Tibial shaft fracture
- Pilon fracture
- Maisonneuve fracture
- Tibia fracture (peds)
- Ankle fracture
- Foot and toe fractures
Foot and Toe Fractures
Hindfoot
Midfoot
Forefoot
Evaluation



- Ottawa Ankle Rules (sen 96-99% for excluding fracture)
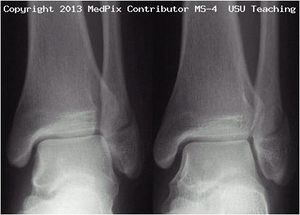
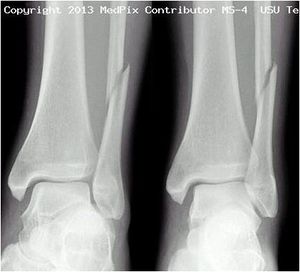
- 3 views:
- AP: Best for isolated lateral and medial malleolar fractures
- Oblique (mortise)
- Best for evaluating for unstable fracture or soft tissue injury
- At a point 1 cm proximal to tibial plafond space between tib/fib should be ≤6mm
- Lateral: Best for posterior malleolar fractures
- consider proximal tib/fib films and talus fractures
Classification (Danis-Weber System)
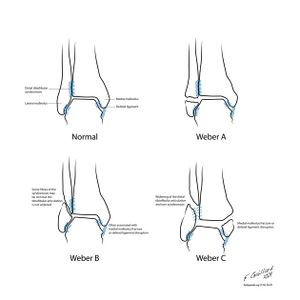
- system based on level of the fibular fracture and characterizes stability of fracture
- tibial plafond and the two malleoli is referred to as the ankle "mortise" (or talar mortise)
Type A
- fibula fracture below ankle joint/distal to plafond
- medial malleolus often fractured
- tibiofibular syndesmosis intact
- usually stable: occasionally requires ORIF
Type B
- fibula fracture at the level of the ankle joint/at the plafond
- can extend superiorly and laterally up fibula
- tibiofibular syndesmosis intact or only partially torn
- no widening of the distal tibiofibular articulation
- medial malleolus may be fracture
- possible instability
Type C
- fibula fracture above the level of the ankle joint/proximal to plafond
- tibiofibular syndesmosis disrupted with widening of the distal tibiofibular articulation
- medial malleolus fracture
- unstable: requires ORIF
Management & Disposition
- Determined by stability of fracture:
- Stable, nondisplaced, isolated malleolar fracture: Splint or cast, early wt bearing, RICE
- Unstable or displaced fracture: Requires ORIF, ortho consult, reduce and splint
Isolated lateral malleolar fracture
- If stable (see Weber classification) treat like severe Ankle Sprain
- Signs of instability:
- Displacement >3mm
- Associated medial malleolus fracture
- Signs of medial (deltoid) ligament disruption such as medial swelling, ecchymosis, or TTP
- Widening of medial clear space (suggests deltoid ligament injury)
Isolated medial or posterior malleolar fracture
- Must rule-out other injuries
- If non-displaced, isolated:
- Short-Leg Posterior Splint (ankle at 90o)
- Non-weight bearing
- Refer to Ortho in 5-7d
Lateral malleolar fracture with deltoid injury OR bimalleolar OR trimalleolar fracture
- Short-Leg Posterior Splint (ankle at 90o)
- Immediate reduction or ortho consult in ED
See Also
- Ankle (Main)
- Ankle Sprain
- Ankle Fracture (Peds)
- Ottowa Ankle Rules
- Maisonneuve Fracture
- Pilon Fracture
- Fracture (Main)
- Splinting
References
, Uptodate, Medpix Radiology Teaching Files (Images by Dr. Timothy Sanders)
- http://radiopaedia.org/articles/weber_ankle_fracture_classification (Images by Dr. Frank Gaillard; CC SA NC BY licence)
- Ottawa Ankle Rules - http://www.ncbi.nlm.nih.gov/pubmed?term=12595378