We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Acute gastric dilation
From WikEM
Contents
Background
- Rare event
- Invariable leads to necrosis with or without perforation
- Most commonly a post-operative complication
Etiologies
- Post-operative complication (Nissen flundoplication)
- Occurs after binge eating episodes, typically in those with an eating disorder
- Anorexia nervosa
- Bulimia nervosa
- Also Psychogenic polyphagia
- Mechanical obstruction
- Pyloric stenosis
- Stricture/adhesions
- SMA syndrome
- Gastric volvulus
- Other etiologies including Diabetes mellitus, trauma, spinal conditions
Pathogenesis
- Intragastric pressure >20mmHg leads to impaired intramural blood flow and mucosal necrosis
- Gastric volumes greater than 4 liters lead to regular mucosal tears
- Patients with pathologic eating disorders can have larger gastric volumes at baseline
- Acute massive gastric dilation is an extreme form (intragastric pressure >30)
Clinical Features
- Emesis is typical symptom in 90% of cases
- Inability to vomit seen in massive distention
- Other features include:
- Abdominal distention
- Abdominal pain
- Signs of peritonitis after perforation
Differential Diagnosis
Nausea and vomiting
Critical
Emergent
- Acute radiation syndrome
- Acute gastric dilation
- Acetaminophen toxicity
- Adrenal insufficiency
- Appendicitis
- Aspirin toxicity
- Bowel obstruction/ileus
- Carbon monoxide poisoning
- Cholecystitis
- CNS tumor
- Digoxin toxicity
- Electrolyte abnormalities
- Elevated ICP
- Gastric outlet obstruction
- Hyperemesis gravidarum
- Pancreatitis
- Peritonitis
- Ruptured viscus
- Testicular torsion/ovarian torsion
- Theophyline toxicity
Nonemergent
- Biliary colic
- Cannabinoid hyperemesis syndrome
- Chemotherapy
- Disulfiram effect
- Erythromycin
- ETOH
- Gastritis
- Gastroenteritis
- Gastroparesis
- Hepatitis
- Ibuprofen
- Labyrinthitis
- Migraine
- Motion sickness
- Narcotic withdrawal
- Thyroid
- Pregnancy
- Peptic ulcer disease
- Renal colic
- UTI
Evaluation
- Typical work up for abdominal pain
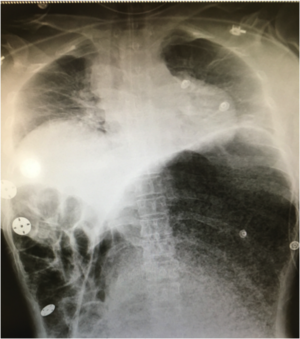
- Upright chest x-ray and abdominal series to assess for free air
- Can identify large distended stomach on x-ray
- CT imaging if safe and indicated
Management
- Nasogastric or orogastric decompression is first line therapy
- Typically a large special tube required which is placed under anesthesiologist supervision in OR
- Resuscitation with fluids and intravenous antibiotics as indicated
- If conservative measures fail or gastric infarction suspected, surgical intervention mandatory
Disposition
- Patient may require emergent surgical decompression
- If improvement with non-operative decompression, may require admission for continued monitoring
Complications
- Bowel necrosis with or without perforation
- Abdominal compartment syndrome
- Sepsis/Septic shock
- If gastric necrosis and/or perforation not recognized and treatment delayed, mortality reaches 80%
See Also
External Links
References
- Dewangan M, Khare MK, Mishra S, and Marhual JC. Binge eating leading to acute gastric dilation, ischemic necrosis and rupture. Journal of Clinical and Diagnostic Research." 2016; 10(3): 6-7.
- Lunca S, Rikkers A, and Stanescu A. Acute massive gastric dilation: Severe ischemia and gastric necrosis without perforation. Romanian Journal of Gastroenterology'. 2005; 14(3): 279-283.
- Santos T, Freitas C, and Pinto-de-Sousa J. Gastric wall ischemia following massive gastric distention due to pyloric stenosis: a case report. Journal of Surgical Case Reports. 2016; 2: 1-3.