We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Tricyclic antidepressant toxicity
From WikEM
Contents
Background
- Abbreviation: TCA
- Used in depression and neuropathic pain
- Serious toxicity is almost always seen within 6hr of ingestion
- Coingestants often increase severity of toxicity
- Cocainecan produce the same sodium blockade effect and exacerbate a TCA overdose
Ingestion amount
- <1mg/kg: Nontoxic
- >10mg/kg: Life-threatening
- >1gm: Commonly fatal
Clinical Features
- Na Channel Blockade
- Negative inotropy, heart block, hypotension, ectopy
- Anti-Histamine Effects
- Sedation, coma
- Anti-Muscarinic Effects
- Central
- Agitation, delirium, confusion, hallucinations
- Slurred speech, ataxia
- Sedation, coma
- Seizures
- Peripheral
- Mydriasis, decreased secretions, dry skin, ileus, urinary retention
- Tachycardia, hyperthermia
- Central
- Alpha1 Receptor Blockade
- Sedation, orthostatic hypotension, miosis
- Inhibition of amine reuptake
- Sympathomimetic effects
- Myoclonus, hyperreflexia
- Serotonin Syndrome (only when used in combination with other serotonergic agents)
Differential Diagnosis
Anticholinergic toxicity
- Medications
- Atropine
- Antihistamines
- Antidepressants
- Antipsychotics
- Muscle relaxants
- Anti-Parkinsonians
- Plants
- Jimson weed (Devil's trumpet)
- Amanita mushroom
Sodium Channel Blockade Toxidrome
- Phenothiazines
- Antihistamines
- Sotalol
- TCAs
- Antipsychotics
- Cocaine
- Anti-spasmodics, cyclobenzaprine
- Chloroquine
- Anti-malarials
- Class Ib antiarrhythmics
- Local anesthetic systemic toxicity
Evaluation
- Serious toxicity
- Conduction delays, SVT, V-tach, hypotension
- Respiratory depression
- Seizures
- Pulmonary Edema
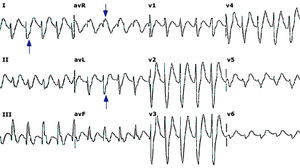
- ECG
- Sinus Tachycardia (most frequent dysrhythmia)
- PR, QRS, QT Prolongation
- Abnormal QRS morphology (deep slurred S wave in I and AVL)
- Threshold of QRS>100 for seizures
- Threshold of QRS>160 for ventricular dysrhymthmias
- RBBB
- Right axis deviation (of terminal 40ms)[1]
- Terminal R wave in aVR, S wave in I/aVL
- R/S > 0.7
- Otherwise, more simply put, tall R wave in aVR
- Brugada pattern (15%)[2][3]
Management
GI Decontamination
- Gastric lavage if <1hr after ingestion
- Activated charcoal 1gm/kg x1
Cardiac Toxicity[4]
Sodium Bicarbonate
- Indications:
- QRS >100ms, terminal RAD >120 deg, Brugada pattern, ventricular dysrhythmias
- Initial Dosing:
- Give 1-2 mEq/kg as rapid IVP; may repeat as necessary (stop if pH > 7.50-7.55)
- May give as 3ampules (132 mEq) of 8.4% NaHCO3
- Infusion Dosing[5]
- Mix 125-150 mEq of NaHCO3 in 1L of D5W; infuse at 250 mL/hr
- Treatment Goal:
- QRS <100ms
- pH 7.50-7.55
- May continue for 12-24hrs due to the drugs redistribution from tissue
- Treatment Monitoring
- Monitor for volume overload, hypokalemia, hypernatremia, metabolic alkalosis
Hyperventilation
- Consider in patients unable to tolerate NaHCO3 (renal failure, pulm/cerebral edema)
- Hyperventilate to pH of 7.50 - 7.55 (same as bicarb administration)
Lidocaine
- At 1.5mg/kg, consider lidocaine for ventricular dysrhythmias if NaHCO3 alone is ineffective
- NOTE
- avoid IA, IB, IC antiarrhythmics, Beta-Blockers, and Calcium Channel Blockers
Phenytoin
- Consider for ventricular dysrhythmias resistant to NaHCO3 and lidocaine
Synchronized cardioversion
- Appropriate in patients with persistent unstable tachydysrhythmias
Seizures
- Benzodiazepines are 1st line
- Barbituates or propofol are 2nd line
- Phenytoin ineffective as no seizure focus in brain
Hypotension
- After repeat fluid boluses and with sodium load from NaHCO3 norepinepherine should be the first line vasopressor
- ECMO is a successful adjunct for refractory hypotension after maximal therapy has failed
- May also consider hypertonic 3% saline for refractory hypotension
Dialysis
Not useful for enhancing elimination due to the large volume of distribution and high lipid solubility
Disposition
- Consider discharging patients who remain asymptomatic after 6hr of observation
- Patients with decreased level of consciousness or seizures should be admitted to ICU
See Also
Video
References
- ↑ Liebelt EL, Francis PD, Woolf AD. ECG lead aVR versus QRS interval in predicting seizures and arrhythmias in acute tricyclic antidepressant toxicity. Ann Emerg Med. Aug 1995;26(2):195-201
- ↑ Goldgran-Toledano D, Sideris G, Kevorkian JP. Overdose of cyclic antidepressants and the Brugada syndrome. N Engl J Med. May 16 2002;346(20):1591-2
- ↑ Monteban-Kooistra WE, van den Berg MP, Tulleken JE. Brugada electrocardiographic pattern elicited by cyclic antidepressants overdose. Intensive Care Med. Feb 2006;32(2):281-5
- ↑ Thanacoody HK, Thomas SH. Tricyclic antidepressant poisoning: cardiovascular toxicity. Toxicol Rev. 2005;24(3):205-14
- ↑ Seger DL, Hantsch C, Zavoral T, Wrenn K. Variability of recommendations for serum alkalinization in tricyclic antidepressant overdose: a survey of U.S. Poison Center medical directors. J Toxicol Clin Toxicol. 2003;41(4):331-8