


Volunteer Fire Fighter Dies after Falling From a Rope –Minnesota
 ShareCompartir
ShareCompartir
 Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
F2011-12 Date Released: October 5, 2011
Executive Summary
On May 23, 2011, a 35-year-old male volunteer fire fighter (victim) died after falling from a rope he was climbing after the conclusion of a ropes skills class. The department was conducting a ropes and mechanical advantage haul systems training session that consisted of classroom and practical skills intended to provide the fire fighters rope skills. The drill had concluded and the students were in the process of breaking down the drill site and putting the equipment away. The victim and two fire fighters were standing in front of the tower ladder when the victim decided to climb one of two suspended ropes in an attempt to access the other suspended rope. The victim was climbing up a rope that had been used to demonstrate rope haul systems and attempted to grab another rope out of his reach. The victim likely lost his grip on the rope and fell to the asphalt pavement striking his head. Emergency medical aid was administered by fellow fire fighters and he was transported to a local hospital where he died from his injuries.
The medical examiner reported the cause of death as blunt force head trauma.

Training Site
(Photo courtesy of fire department)
Contributing Factors
- Lack of a safety officer
- Lack of proper personal protective equipment
- Student to instructor ratio
Key Recommendations
- Fire departments should ensure that a qualified safety officer (meeting the qualifications defined in NFPA 1521) is appointed in practical skills training environments.
- Fire departments should ensure that minimum levels of personal protective equipment are established for practical skills training environments (as defined in NFPA 1500).
- Fire departments should ensure that sufficient instructors or assistant instructors are available for the number of students expected to participate in practical skills training evolutions.
Additionally, states, municipalities and authorities having jurisdiction should:
- Take steps to ensure that ropes and equipment used in emergency services practical skills training are inspected and records are kept on the purchase, use and inspection of the ropes and equipment (as defined in NFPA 1500 4.6.5) .
Introduction
On May 23, 2011, a 35-year-old male volunteer fire fighter (victim) died after falling from a rope he was climbing after the conclusion of a rope skills class. The victim had climbed up a rope that had been used to demonstrate rope haul systems and was attempting to grab another rope out of his reach (see photo 1). The victim likely lost his grip on the rope and fell to the ground striking his head on the asphalt. On May 25, 2011, the U.S. Fire Administration notified the National Institute for Occupational Safety and Health (NIOSH) of this incident. On June 5 – June 9, 2011, a safety engineer and a safety and occupational health specialist from the NIOSH Fire Fighter Fatality Investigation and Prevention Program in Morgantown WV traveled to Minnesota to investigate this incident. The NIOSH investigators conducted an opening meeting with the city administrator and the fire chief. The NIOSH investigators also met with representatives of the Minnesota State Colleges and Universities and the local technical college that provided the training for the department. Note: The Minnesota Board of Firefighter Training and Education was established by the Minnesota Legislature as defined in Minnesota Statute 299N. Its function is to: (1) review fire service training needs and make recommendations on training to Minnesota fire service organizations; (2) establish standards for educational programs for the fire service and develop procedures for continuing oversight of the programs; and (3) establish qualifications for fire service training instructors in programs and establish standards under which reimbursement will be provided for training and education. NIOSH investigators reviewed surveillance video that recorded part of the training session with the local police department. The NIOSH investigators visited the incident scene and conducted interviews with officers and fire fighters of the involved department who were present during the training. The NIOSH investigators reviewed the fire department's standard operating guidelines, the victims' training records, photographed the incident scene and spoke with the county medical examiner.
Fire Department
The victims' department is a volunteer department that has 1 station with 26 members that serve a population of approximately 7,725 residents within an area of about 100 square miles and responds to approximately 141 emergency incidents per year. The department does not provide emergency medical services but does provide vehicle extrication at motor vehicle accidents within the department's response area. The department receives its funding directly from the city.
The fire department provides annual physicals for new members only and provides face piece fit testing annually for its members. Following this incident, the fire department implemented a new policy where a Safety Officer was designated and served at all hands-on training sessions.
Training and Experience
The victim had 1 year and five months of service with the department, and had successfully completed Fire Fighter 1 and Fire Fighter 21 training as well as hazardous materials operations level training and certified first responder training.
The victims’ fire department requires members to attain Fire Fighter 1 and 2 training (approximately 240 hours) within one year of membership. The department provides two drills per month and members must attend 60% of the drills per year. The department also provides annual driver training with a simulator and actual driver training on a cone course. The department contracts with the local technical college to provide fire fighter training for its members. Members are on probation for one year after joining the department.
Note: Fire Fighter 1 and 2 training met the criteria for National Fire Protection Association (NFPA) 10011, Standard for Fire Fighter Professional Qualifications, Fire Fighter I and Fire Fighter II.
Equipment and Personnel
The department had the following equipment in service:
- Engine 1, 1500 GPM Pumper
- Engine 2, 1250 GPM Pumper
- Engine 3, 1250 GPM Pumper
- Ladder 1, 95’ Aerial Platform
- Tender 1, 1800 gallon Tanker
- Tender 2, 1800 gallon Tanker
- 3 Grass Fire Rigs
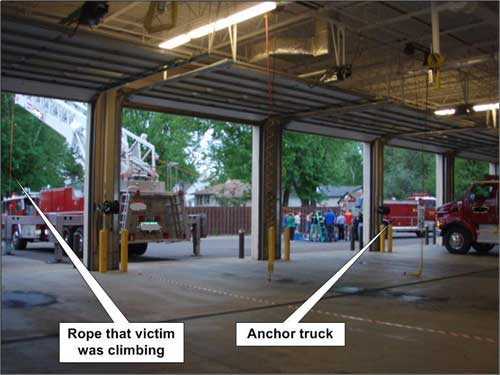
Photo 1. Training site in front of firehouse.
(Photo courtesy of fire department)
Personal Protective Equipment
The victim was reported to be wearing civilian clothes with no PPE.
Weather/Road Conditions
At the time of the incident (approximately 2130 hours), the weather was clear with an approximate temperature of 64°F. The relative humidity was 73% and the wind was NNW at 4.6 mph.2
Investigation
On May 23, 2011, a 35-year-old male volunteer fire fighter (victim) died after falling from a rope he was climbing after the conclusion of a rope skills class. The victim had climbed up a rope that had been used to demonstrate rope haul systems and was attempting to grab another rope out of his reach. The victim likely lost his grip on the rope and fell to the asphalt pavement striking his head. Emergency medical aid was administered by fellow fire fighters and he was transported to a local hospital where he died from his injuries.
The incident occurred in front of the victim's fire station on a drill site consisting of a 95 foot aerial platform elevated approximately 20-30 feet in the air and a tanker/tender used as an anchor point for the rope system (see photo 2). The department was conducting a ropes and mechanical advantage haul systems drill that consisted of classroom and practical skills intended to provide the fire fighters rope skills. The training was provided by a contract agreement with the local technical college. The drill was a continuation of a two-day 8-hour rope skills training session that was provided by the technical college (the first four hour ropes and knots and rigging class had been held approximately two weeks prior and most of the students including the victim had attended both sessions). The instructor for the class was an adjunct instructor for the college and also a fire fighter for a neighboring large city. The college had originally sent two instructors but one of the instructors had to cancel at the last minute due to an emergency. The instructor and the chief of the department decided to continue the class since most of the training was classroom with the exception of a demonstration of the ropes and haul system. The first portion of the second four hour training session was held in the classroom at the fire station and the demonstrative training was held outside on the fire station apron. The training consisted of the demonstration of a number of different haul system configurations designed to create a mechanical advantage using ropes and pulleys to lift objects. Fire fighters interviewed during the investigation stated that the training was focused on the haul system that was built at the anchor end of the rope system at the tanker truck (Photo 1). The fire fighters were rotated through different activities, including viewing the rigging points and pulleys and setting up the systems such as the hauling and anchor points and the safety rope. All of the fire fighters and officers interviewed acknowledged that the instructor kept the students attention focused on the training activities. There were 19 students participating in the training.
The drill had concluded and the students were in the process of breaking down the drill site and putting the equipment away. Fire fighters were attempting to lower the aerial platform but were having difficulty getting the truck’s engine started. A fire fighter had attempted unsuccessfully to start the engine on the aerial platform and was receiving help from another fire fighter to diagnose why he couldn’t start the engine. They discovered that the pull stop for the engine was still engaged and then corrected and started the engine. The victim and two fire fighters were standing in front of the tower ladder when the victim (without PPE) decided to climb one of two ropes suspended from the bottom of the aerial platform in an attempt to access the other suspended rope. The instructor and the fire chief saw the victim on the rope and both of them called for him to stop and get down. The victim then apparently lost his grip on the rope and fell head first approximately 6-8 feet to the pavement. The instructor and other fire fighters began emergency medical procedures and the victim was transported to a local hospital where he died from his injuries.

Photo 2. Victim fell off of one of the two ropes hanging from the tower ladder.
(Photo courtesy of fire department)
Contributing Factors
Occupational injuries and fatalities are often the result of one or more contributing factors or key events in a larger sequence of events that ultimately result in the injury or fatality. NIOSH investigators identified the following items as key contributing factors in this incident that ultimately led to the fatalities:
- Lack of a safety officer
- Lack of proper personal protective equipment
- Student to instructor ratio
Cause of Death
According to the medical examiner, the cause of death was due to blunt force head trauma.
Recommendations
Recommendation #1: Fire departments should ensure that a qualified safety officer is appointed in practical skills training environments.
Discussion: Fire departments should ensure that a qualified safety officer (meeting the qualifications defined in NFPA 1521)3 is appointed in practical skills training environments. NFPA 1521 chapter 5.3.4 also states "the health and safety officer shall ensure that safety supervision is provided at all live training activities". 3 The safety supervision should be provided throughout the training and continue throughout breakdown and termination of the training. Fire departments should consider appointing multiple safety officers or assistant safety officers when the size or complexity of the training is too great for a single safety officer. Ascending a fixed rope is a skill that is performed by Level 1 (Operations Level) Rope Rescue Technicians and should not be attempted by individuals in a rope skills or awareness level class.4 A qualified safety officer can prevent students from attempting a skill beyond their level of training.
During this incident, all of the fire fighters interviewed stated that ascending and/or repelling skills were not expectations of the ropes skills class. The training was supposed to be classroom activities followed by demonstrative activities using the rope haul systems. The demonstrative activities involved student participation in pulling ropes and connecting anchor points and other activities. A qualified safety officer could have given the students a safety briefing before the training began that explained the activities, participation levels and the minimum PPE (personal protective equipment) necessary for the drill. Fire fighters were attempting to lower the aerial platform but were having difficulty getting the truck's engine started. A fire fighter had attempted unsuccessfully to start the engine on the aerial platform and was receiving help from another fire fighter to diagnose why he couldn't start the engine. When the other fire fighters could not lower the aerial platform right away the victim decided to climb the rope. The activities that the victim and other fire fighters were engaged in during the break down phase of the drill session could have been monitored by a safety officer and other methods of retrieving the rope such as lowering the aerial or using a pike pole suggested. Maintaining a safety discipline is a responsibility of all members and the safety officer can assist the fire chief in ensuring that the discipline is maintained throughout the drill and during the breakdown of equipment and cleanup. Note: maintaining the safety discipline on a drill site after the drill is over and throughout breakdown and clean-up is the same as maintaining the safety discipline on a fire ground incident throughout the fire and salvage and overhaul. After the drill is over the students might tend to relax their guard just like at a fire incident, and allow the discipline of safety to take a secondary priority in seemingly common activities such as salvage, overhaul and clean-up. The department involved in this incident has instituted a department safety officer since this incident.
Recommendation #2: Fire departments should ensure that minimum levels of personal protective equipment are established for practical skills training environments.
Discussion: Personal protective equipment should be utilized whenever there is a chance of injury from falling objects or other hazards such as injuries from falls, rope burns and/or contact with equipment and tools. During practical skills training minimum levels of PPE should be established by the instructor and re-enforced by the safety officer as well as all members participating in the drill. Proper PPE should be worn throughout the training, during the breakdown of the equipment after the training or until all equipment is placed back into service. Instructors can include the PPE requirements and safety concerns in any written correspondence that may be distributed before the training begins.
During this incident, the victim and other fire fighters were trying to retrieve a dangling rope and the victim (with the assistance of other fire fighters) climbed a second rope attempting to retrieve it. The victim fell from an elevation of reportedly less than 10' and struck his head on the asphalt. If the victim had been wearing a helmet his injuries would likely have been much less severe.
Recommendation #3: Fire departments should ensure that sufficient instructors or assistant instructors are available for the number of students expected to participate in practical skills training evolutions.
Discussion: Practical skills training require a lower instructor to student ratio than classroom training. When planning for practical skill training, fire departments should insure that a sufficient number of instructors are available to deliver the required training and maintain the safety discipline of the students. The proper student to instructor ratio when teaching practical skills is recommended to be 5:1.5 The instructor must pay attention to detail when planning and conducting drills where students may face a risk of injury. When conducting practical drills, many variables come into play and many things can go wrong, resulting in an injury to a student. One way the instructor can help minimize that possibility is to pay special attention to every detail of the drill. Mentally walking through the evolution during the planning session and drawing on his/her own experiences or case reports of actual incidents can help develop your awareness of what might potentially go wrong. Additional fire service instructors should be employed at training sessions where the following conditions are present:
- Extreme temperatures are expected
- Large groups of people are participating
- Training will take place over a long duration
- Training involves complex evolutions and procedures where additional instruction and safety oversight may be valuable.5
The fire service instructor should be aware of factors that could influence the learning process and be able to adjust the presentation to changing circumstances such as safety, limited resources, presentation locations, unsafe behavior and others so that the objectives of learning outcome are achieved.6 Every student participating in training has a stake in ensuring his or her own personal safety. Each student is responsible for his or her own actions as well as the actions of other crew members, training team members, and fellow students when it comes to addressing hazardous conditions. Students should be knowledgeable about the training to take place and should meet all of the prerequisites specified before participating in the drill. This can be accomplished through formal training or by individual study. Students should also adhere to all PPE requirements specified for the evolution and wear all SCBA or other assigned safety devices. Observance of all safety instructions and safety rules throughout the training session will assist in maintaining the overall safety profile of the training session.5
During this incident, the training session was scheduled to have two instructors from the local technical college. One of the instructors experienced an emergency and was not able to attend. Since the delivery of the training was focused on classroom and demonstrative skills, the lead instructor from the college and the fire chief elected to provide the training with the instructor and the fire chief assisting him. The number of fire department personnel (19 students) and the size of the drill site allowed for fire fighters to be spread out and possibly not under the control or direction of the lead instructor or the chief at all times.
Additionally, states, municipalities and authorities having jurisdiction and fire departments should:
Recommendation #4: States, municipalities and authorities having jurisdiction and fire departments should take steps to ensure that ropes and equipment used in emergency services practical skills training are inspected and records are kept on the purchase, use and inspection of the ropes and equipment.
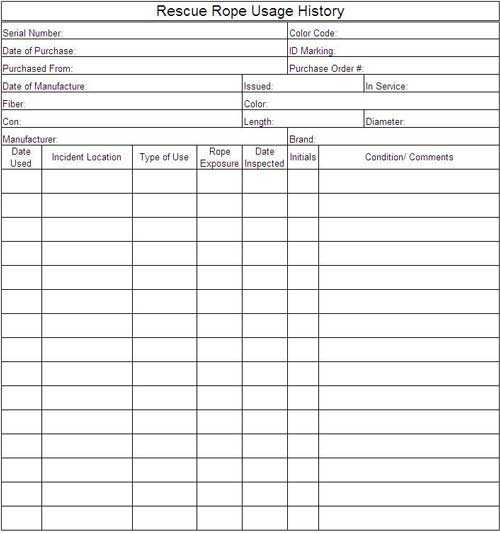
Discussion: When life safety rope is purchased, the authority having jurisdiction should ensure that the product label(s) with the information as specified in 5.1.1 and 5.2.1 of NFPA 1983, Standard on Life Safety Rope and Equipment for Emergency Services7, is attached and remains with the rope until placed in service. When the product label is removed from the rope, the label should be retained in the authority's permanent rope records. It is very important that the information on the product label (s) and the information required in 5.2.1 to be supplied by the manufacturer reach the persons who will actually be using the rope. It is useless for the supply personnel or equipment officer to remove the product label and other pertinent information and simply retain them in the rope record file. The persons who potentially will be using the rope need to be provided with all the information available. Copies of the product label (s) and other pertinent information should be maintained with the rope wherever the rope is in-service awaiting use so that potential users can consult the information. Ropes can be damaged in use by high impact stresses, impact loading situations, abrasion, kinking, heat, and exposure to chemicals and other products. Ropes should be inspected by a qualified person before and after each operation and carefully stored between each use. Records should provide a history of each rope and should call for regular inspection and replacement as necessary (see figure 1, Rescue Rope Usage History). Any rope that fails to pass inspection or has been impact-loaded should be destroyed immediately.7 The destruction of the rope means that it should be removed from service and altered in such a manner that it could not be mistakenly used as a life safety rope. This alteration could include disposal or removal of identifying labels and attachments and cutting the rope into short lengths that could be used for utility purposes.8 It is recommended that departments establish an inspection program and shelf-life criteria for their ropes based on the conditions and environments encountered in their respective operations. 7 NFPA 1500 chapter 4.6.58 states "The fire department shall ensure that inspection, maintenance, repair, and service records are maintained for all vehicles and equipment used for emergency operations and training."
During this incident, the life safety rope was provided under contract by the local technical college. Although the rope and equipment's performance was not a factor in the incident, the rope's inspection record was not available. At the time of the incident, the local technical college required the ropes to be inspected but the observation was not recorded.
References
- NFPA [2008]. NFPA 1001 standard for firefighter professional qualifications. 2008 ed. Quincy, MA: National Fire Protection Association.
- Weather Underground [2011]. Weather history for Minnesota, May 23, 2011. [http://www.wunderground.com/history/airport/KCBG/2011/5/23/DailyHistory.html?req_city=NA&req_state=NA&req_statename=NA] Date Accessed: June 15, 2011.
- NFPA [2008]. NFPA 1521 standard for fire department safety officer. 2008 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2008]. NFPA 1006 chapter 6.15, standard for technical rescuer professional qualifications. 2008 ed. Quincy, MA: National Fire Protection Association.
- IAFC [2009]. Fire Service instructor: principles and practice. Sudbury, MA: Jones and Bartlett Publishers.
- NFPA [2007]. NFPA 1041, A.4.4.4, A.4.4.5 standard for fire service instructor professional qualifications. 2007 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2006]. NFPA 1983, A.5.1.1.8 standard on life safety rope and equipment for emergency services. 2006 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2007]. NFPA 1500 standard on fire department occupational safety and health program. Quincy, MA: National Fire Protection Association.
Investigator Information
This incident was investigated by Stephen Miles, Safety and Occupational Health Specialist and Timothy Merinar, Safety Engineer, with the Fire Fighter Fatality Investigation and Prevention Program, Surveillance and Field Investigations Branch, Division of Safety Research, NIOSH located in Morgantown, WV. An expert technical review was provided by Brian P. Kazmierzak, EFO, MABAS Division 201 Tactical Rescue Team Task Force Leader. A technical review was also provided by the National Fire Protection Association, Public Fire Protection Division.
Additional Information
Minnesota Board of Fire Fighter Training and Education, as an independent state agency the MN Board of Firefighter Training and Education (MBFTE) is responsible for standards and licensing of the fire service in Minnesota; their mission is to identify needs, develop and enforce procedures and assure quality education, which contribute to the safety and well-being of the people of Minnesota. http://mn.gov/mbfte/index.html (Link updated 8/12/2013)
Disclaimer
Mention of any company or product does not constitute endorsement by the National Institute for Occupational Safety and Health (NIOSH). In addition, citations to Web sites external to NIOSH do not constitute NIOSH endorsement of the sponsoring organizations or their programs or products. Furthermore, NIOSH is not responsible for the content of these Web sites.
The National Institute for Occupational Safety and Health (NIOSH), an institute within the Centers for Disease Control and Prevention (CDC), is the federal agency responsible for conducting research and making recommendations for the prevention of work-related injury and illness. In 1998, Congress appropriated funds to NIOSH to conduct a fire fighter initiative that resulted in the NIOSH “Fire Fighter Fatality Investigation and Prevention Program” which examines line-of-duty-deaths or on duty deaths of fire fighters to assist fire departments, fire fighters, the fire service and others to prevent similar fire fighter deaths in the future. The agency does not enforce compliance with State or Federal occupational safety and health standards and does not determine fault or assign blame. Participation of fire departments and individuals in NIOSH investigations is voluntary. Under its program, NIOSH investigators interview persons with knowledge of the incident who agree to be interviewed and review available records to develop a description of the conditions and circumstances leading to the death(s). Interviewees are not asked to sign sworn statements and interviews are not recorded. The agency's reports do not name the victim, the fire department or those interviewed. The NIOSH report's summary of the conditions and circumstances surrounding the fatality is intended to provide context to the agency's recommendations and is not intended to be definitive for purposes of determining any claim or benefit.
- Page last reviewed: November 18, 2015
- Page last updated: October 15, 2014
- Content source:
- National Institute for Occupational Safety and Health Division of Safety Research