


Career Fire Fighter/Emergency Medical Technician Dies and Paramedic is Injured in a Three-Vehicle Collision - Nebraska
 ShareCompartir
ShareCompartir
 Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
F2003-33 Date Released: May 31, 2005
SUMMARY
On August 6, 2003, a 43-year-old career fire fighter/emergency medical technician [the victim] died after the ambulance he was driving was struck from behind and pushed into a straight truck. The victim and a lieutenant/paramedic were conducting a non-emergency transport between two hospitals. The ambulance was traveling through a highway workzone and as the ambulance driver slowed down to move around a line painting crew, a tractor semi-trailer struck the rear of the ambulance and pushed it into the straight truck (Photo 1). Although the victim was using the vehicle occupant restraint, the front cab sustained such extensive damage that he was fatally injured. The lieutenant/paramedic and a patient, who had been riding in the ambulance patient compartment, were also injured during the collision. NIOSH investigators concluded that to help prevent similar incidents:
- state department of highways and highway construction companies should consider the use of signs and warnings supplemental to those specified by the Manual on Uniform Traffic Control Devices (MUTCD) when conducting mobile operations (such as line painting)
- trucking companies should train drivers to maintain safe following distances and to be aware of work zone hazards and slowing traffic
Fire departments and emergency medical service (EMS) providers should:
- ensure that EMS workers use the patient compartment vehicle occupant restraints whenever possible
- consider using shoulder straps with occupant restraints on patient cots to limit the movement of the patient from the cot during a vehicle crash.
Ambulance manufacturers, EMS providers, and researchers should:
- develop and evaluate occupant protection systems designed to provide crash protection for EMS workers and the mobility necessary to access patients and equipment within ambulance patient compartments.

|
|
Photo 1. Ambulance was pushed into rear of straight truck during the crash.
|
INTRODUCTION
On August 6, 2003, a 43-year-old male career fire fighter/emergency medical technician (EMT) died and a 47-year-old paramedic was injured when their ambulance was struck by a tractor semi-trailer and pushed into the back of a straight truck. On August 8, 2003, the U.S. Fire Administration (USFA) notified the National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research of this incident. On October 15, 2003, a Safety and Occupational Health Specialist and a Safety Engineer investigated the incident. The NIOSH team interviewed the Chief and members of the department. They reviewed standard operating guidelines (SOGs), fire department photographs, reports from the Nebraska State Patrol and the County Sheriff, training records of the victim, the death certificate, and data from the 2003 Fatality Analysis Reporting System (FARS) data base.
Background The combination department is comprised of 39 career and 36 volunteer fire fighter/EMTs, and serves a population of approximately 35,000 in an area of about 370 square miles. The department has three fire stations.
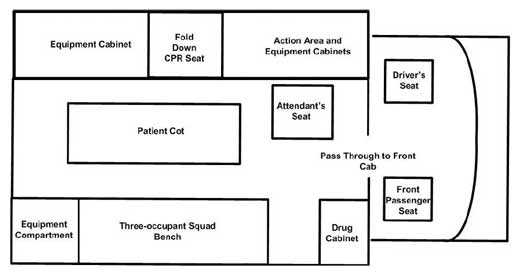
Equipment The vehicle involved in this incident was a 2002 Type IIIa ambulance with a 159-inch wheelbase and 168-inch patient compartment. It was powered by a 7.3 liter turbo-diesel engine and automatic transmission. The gross vehicle weight listed for the vehicle was 14,050 pounds: 4,600 pounds for the front axle and 9,450 pounds for the rear. Actual weight of the vehicle at the time of the crash could not be established. It was equipped with an anti-lock braking system and three-point lap and shoulder seat belts for the front seat occupants. The patient compartment of the ambulance was configured with five seating positions, each equipped with two-point lap belt-type restraints. (Diagram 1) These positions included a rear-facing high-backed attendant’s seat, a squad bench with accommodation for three occupants, and a fold-down CPR seat. Up-to-date ambulance maintenance and inspection logs were maintained by the department.
Other Vehicles Involved in Crash The vehicle that hit the rear of the ambulance was a tractor semi-trailer combination, consisting of a 2000 model year, three-axle conventional cab tractor with a 50-foot semi-trailer. (Photo 2) After the incident, the tractor semi-trailer weighed 79,300 pounds. This vehicle was being operated by a 46 year-old driver who possessed a valid Commercial Driver’s License. Investigators were not able to determine his experience or training history. No vehicle defects for this vehicle were noted by the police investigators.
The vehicle that the ambulance was pushed into was a 1998 two-axle straight truck chassis mounted with a cargo van body; it weighed 30,300 pounds. Police investigators noted no defects for this vehicle.
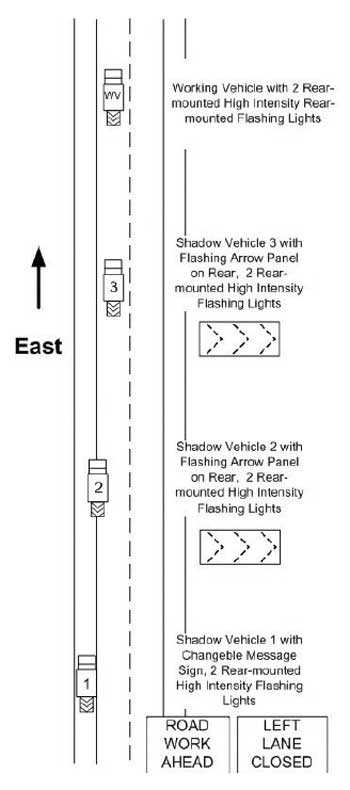
Street Conditions/Weather The ambulance was traveling east on an interstate divided highway comprised of two eastbound and two westbound lanes with paved shoulders. The weather was clear and sunny and the road surface was dry. The section of highway was located within a 14-mile repaving project that was nearly complete. The road surface was new asphalt. A mobile line painting crew was operating within the project area. The western approach to the project was marked according to the Manual on Uniform Traffic Control Devices (MUTCD)1 with permanent signs indicating a 75 mph maximum speed limit, road work for the next 14 miles, and the doubling of fines for exceeding the speed limit. Temporary traffic control devices including speed limit reduction signs were posted within the project area depending on the type and location of the construction operation. On the day of the incident, a message board sign was in place at the beginning of the project area advising motorists of a left lane closure, to use caution, and that slow traffic was possible. At the time of the incident, the mobile operation was a little over 7 miles from the western start of the project. The mobile operation which included a working vehicle and three shadow vehicles at 1000-foot intervals, was set-up as depicted in Diagram 2 and conformed to the MUTCD specifications for mobile operation on multi-lane high-speed roadways. The rearmost shadow vehicle was being driven on the left hand shoulder of the roadway and was equipped with two rear-mounted high intensity flashing lights and a changeable message sign that alternately flashed “ROAD WORK AHEAD” and “LEFT LANE CLOSED.” The second shadow vehicle was driven straddling the roadway edge line and was equipped with two rear-mounted high intensity flashing lights and a flashing arrow sign indicating “merge right.” A third shadow vehicle, being driven directly behind the working vehicle, was equipped with 2 rear-mounted flashing high intensity lights and a flashing arrow sign indicating “merge right”. The working vehicle was equipped with two rear-mounted high intensity flashing lights.
Training and Certifications The department requires all career staff to be trained and certified as both a fire fighter and an emergency medical technician (EMT). The victim was a career fire fighter and had completed the department fire fighter training requirements, including National Fire Protection Association (NFPA) Fire Fighter Level I and he was a certified EMT-B (basic). As a State requirement, he had completed 30 hours of continuing education units every three years to maintain his EMT-B certification. The fire department requires a driver to train over a six-month period and requires a driver training rotation on all of the department’s vehicles. The victim had attended a two-hour defensive driving class in 2002, and had a valid driver’s license, which is required by the State to drive fire apparatus. There are no additional State licensing prerequisites for ambulance drivers. The victim had been working as a fire fighter/EMT for eighteen years and had been with the department the entire time.
The lieutenant/paramedic attending to the patient who was injured at the time of the incident was a career fire fighter and certified EMT-P (paramedic). He had completed department fire fighter training requirements and the state-required 60 hours of continuing education units every three years to maintain his EMT-P certification. He had been with the department for 18 years at the time of the incident.
a A Type III ambulance is a cutaway van chassis with integrated modular patient compartment.
INVESTIGATION
On August 6, 2003, a call was received at the fire department from the local hospital requesting an ambulance for a non-emergency patient transport to another hospital located approximately 230 miles away. Due to the long distance of the transport, the hospital also requested a paramedic to provide patient care. The duty officer of the fire department paged the victim and the lieutenant/paramedic, who were both off-duty, to report to the station for a transport. The ambulance arrived at the hospital at 1300 hours. At 1319, the ambulance departed from the hospital with the victim driving and the lieutenant/paramedic attending to the patient. The emergency lights and siren were not activated because this was a non-emergency transport.
During the transport, the lieutenant/paramedic was positioned in the rear-facing attendant’s seat, moving to the bench seat every hour to check the patient’s vital signs. The patient was positioned on the cot with his head elevated and with the cot safety straps fastened across his chest, pelvis, and legs.
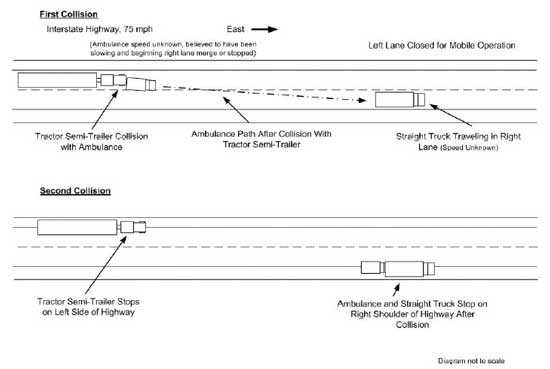
At 1605 hours, while traveling eastbound in the left lane, the ambulance approached the mobile operation engaged in painting lines on the road. Meanwhile, the patient had asked to borrow the lieutenant/paramedic’s mobile telephone. The lieutenant/paramedic unbuckled his seat belt, moved over and sat on the squad bench, and handed his phone to the patient. The patient dialed the phone and talked, while the lieutenant/paramedic returned to the attendant’s seat. As the lieutenant/paramedic was sitting down in the seat he observed through the rear windows of the ambulance a tractor with a semi-trailer quickly approaching. The ambulance had slowed or nearly stopped as it approached the line painting crew and the tractor semi-trailer struck it in the rear. The tractor semi-trailer driver applied the brakes and steered left and the tractor semi-trailer came to a stop with its left wheels on the left shoulder of the road. (Diagram 3) The ambulance which may have been been steering right to merge was pushed approximately 240 feet until it collided with the rear of a straight truck traveling in the right lane. The ambulance and straight truck came to rest on the right shoulder of the road. The collision forces crushed the front of the ambulance and pushed its engine back into the cab (Photo 3). The State Patrol investigators estimated the tractor semi-trailer’s speed at 61 mph at the time the driver applied the brakes.
During the collision, the lieutenant/paramedic, in the process of regaining his position on the attendant’s seat, slipped off the curb side seat edge and continued moving toward the driver’s cab. As he did so, he felt his thigh strike the patient-cot. His next memory was that of being wedged in the pass-through to the front cab and lying on top of the patient, who had been ejected from the cot. The patient told the lieutenant/paramedic that because he was laying on top of him, he could not breathe. However the lieutenant/paramedic could not move. A fire had started under the ambulance and according to the lieutenant/paramedic, it was dark and smoky inside the ambulance. A passing motorist stopped to assist. He used a fire extinguisher from one of the crashed trucks to put out the fire. Light entered the ambulance when a motorist and two off-duty EMTs who had been traveling westbound observed the collision, opened the door of the ambulance, and began to remove the patient and the lieutenant/paramedic. Several fire departments responded to the incident and upon arriving at the scene made an assessment of the situation. They decided that the extent of the lieutenant/paramedic’s injuries necessitated that he should be life-flighted to a hospital located 20 miles away from the incident. The patient was transported to the same hospital by a fire department ground ambulance. After the lieutenant/paramedic and the patient had been transported from the scene, several fire department members extricated the victim from the front seat area. The victim was transported to the hospital and pronounced dead at 1657 hours. Although the victim was using the vehicle occupant restraint, the front cab sustained such extensive damage that he was fatally injured. The lieutenant/paramedic suffered several fractures and lacerations. He spent one week in the hospital intensive care unit and an additional five weeks in a rehabilitation facility. The patient suffered no serious injuries.
The physical evidence gathered by the state police investigators indicate that the tractor semi-trailer collided with the ambulance only 2 feet beyond the point at which the semi-trailer’s wheels had been braked to the point of skidding. This suggests that the tractor semi-trailer driver’s attention may have been distracted from driving, or he significantly misjudged either the rate he was overtaking the ambulance, the distance between the ambulance and the tractor semi-trailer, or the braking capacity of the tractor semi-trailer. The police report indicates that the tractor semi-trailer driver was cited for following too closely.
Cause of Death
The death certificate listed the cause of death as blunt force trauma due to a motor vehicle accident.
RECOMMENDATIONS/DISCUSSIONS
Recommendation #1: State department of highways and highway construction companies should consider the use of signs and warnings supplemental to those specified by the Manual on Uniform Traffic Control Devices (MUTCD) when conducting mobile operations (such as line painting).
Discussion: It could not be ascertained whether the tractor semi-trailer driver was aware that he was approaching a mobile work operation and that traffic in front of him would be slowing and merging right. Nor could it be determined if he knew the ambulance was moving slower than his truck. The distance between the point of the tractor semi-trailer collision with the ambulance and the mobile work operation is not known. As previously noted, the western approach to the project was marked with traffic control signs and warnings that conformed to the specifications of the MUTCD. However, within the 7¼ mile distance from the start of the project to the incident site, no other temporary traffic control signs were posted. A vehicle traveling at the posted maximum 75 mph limit would require about 5½ minutes to travel this distance. Also, the signage at the western approach indicated a left lane closure, but did not include information to tell drivers that the closure was due to a mobile operation whose location was continually changing. While the set-up of both the stationary and the mobile traffic control signs conformed to the MUTCD specifications, additional warnings located within the project area could be used to remind motorists that they were still traveling in an active work zone. This information could warn motorists that the work operations were moving and could be encountered at any time while traversing the 14-mile project area. Message board signs could be used to flash warnings that are more descriptive of the operation being conducted, such as “MOBILE OPERATIONS AHEAD”, “SLOW MOVING TRAFFIC” or “LINE PAINTING IN PROGRESS.” These measures could guard against motorists becoming desensitized to the existence of work zone hazards after they have traveled in a designated work zone for several miles without encountering work operations.
Recommendation #2: Trucking companies should train drivers to maintain safe following distances and to be aware of work zone hazards and slowing traffic.
Discussion: A National Transportation Safety Board Safety Recommendation of May 25, 2001, reported that of 1,923 fatalities occurring as a result of rear-end collisions in 1999, 770 involved commercial vehicles (trucks weighing more than 10,000 pounds and motor coaches).2 This represented 40% of the fatal crashes even though commercial vehicles only accounted for 3% of the vehicles. In work zones, commercial vehicles were involved in 62% of the fatal rear-end crashes.
Results of a police reconstruction estimated that the tractor semi-trailer was traveling at a minimum speed of 61 mph when its wheels started to skid. Given that the posted speed limit was 75 mph, the tractor semi-trailer driver may have been slowing as he approached the ambulance. However, the physical evidence reported by the police reconstruction also indicates that the semi-trailer collided with the ambulance only 2 feet beyond the point at which the tractor semi-trailer’s wheels began to skid. This suggests that the tractor semi-trailer driver’s attention may have been distracted or he may have significantly misjudged either the rate he was overtaking the ambulance, the distance between the ambulance and the tractor semi-trailer, or the braking capacity of the tractor semi-trailer. Maintaining safe following distance allows motorists time to adjust to traffic speed and provides sufficient distance for safe stopping and collision avoidance. The rule-of-thumb for safe following distance is one second of space for each 10 feet of vehicle length at speeds below 40 mph. At speeds over 40 mph, add one second.3 For example, a safe distance for the 75-foot long tractor semi-trailer in this incident at speeds over 40 mph would be 8 seconds. If additional space between the ambulance and the tractor semi-trailer had been available, the driver may have been able to slow down or steer away from the collision.
Recommendation #3: Fire departments should ensure that EMS workers use the patient compartment vehicle occupant restraints whenever possible.
Discussion: The patient compartment of the ambulance involved in this incident was configured with five seating positions, each equipped with two-point lap belt-type restraints. The department’s written policies required all occupants of the ambulance to wear the lap-belt occupant restraints while the ambulance was in motion unless they interfered with personnel providing patient care. According to the lieutenant /paramedic, he had ridden restrained in the attendant’s seat for the entire trip except when he had moved to the squad bench to check the patient’s vital signs and hand him the cell phone. He was in the process of resuming his restrained position in the attendant’s seat (Photo 4) when the collision occurred. It should be noted that the lap-belt restraint systems commonly used in ambulances may not allow full access to the patient during treatment for all conditions. For example, when properly used, the squad bench lap belt positions the occupant against the side wall in such a manner that the EMT may not be able to bend forward far enough to access the patient and check vital signs. If the EMT needs to access the cabinets along the opposite wall, the lap-belt must be unbuckled to allow the EMT to stand up. Additionally, if it is necessary to perform CPR or other procedures, such as intubations or insertion of IVs, it may be necessary for the EMT to unbuckle the lap-belt to stand over or kneel at the side of the cot.
Recommendation #4: Fire departments and emergency medical service providers should consider using shoulder straps with occupant restraints on patient cots to limit the movement of the patient from the cot during a vehicle crash.5
Discussion: Although not seriously injured during the collision, the patient was ejected from the cot and came to rest on the patient compartment floor, wedged in the pass-through and underneath the lieutenant/paramedic. Cots used by the department were equipped with occupant restraints that consisted of safety straps for the patient’s chest, abdomen, pelvis, and legs, but did not have shoulder straps. As this incident shows, safety straps across the patient’s body offer little resistance to forward movement induced from collisions. A patient ejected from the cot during a head-on collision is at risk of injury from impacts with the patient compartment bulkhead or an occupant seated in the attendant’s seat. Other patient compartment occupants are at risk of injury if an ejected patient collides with them during a crash.
Recommendation #5: Ambulance manufacturers, EMS providers, and researchers should develop and evaluate occupant protection systems designed to provide crash protection for EMS workers and the mobility necessary to access patients and equipment within ambulance patient compartments.5
Discussion: Currently, ambulance patient compartments are equipped with two-point lap-belt occupant restraints. As previously noted, proper use of these restraints precludes EMS worker mobility in the patient compartment and access to the patient for procedures such as CPR. In a 2003 study of the relative risk for injury in emergency vehicles, over half of the ambulance occupant fatalities occurred to unrestrained patient compartment occupants and unrestrained patient compartment occupants accounted for nearly half of the incapacitating injuries.6 Harness-type restraint systems that afford user mobility are commonly used in military aircraft and civilian air ambulances. Similar systems that allow mobility for workers have been designed for ground ambulances and have been used on a limited scale.4 These systems employ retractor-equipped tethers to connect a harness worn by the EMT to strategic locations on the vehicle structure. The retractor allows occupant mobility by winding the tether on or off of a reel. In a vehicle crash, the retractor automatically locks the reel to limit occupant motion. Although their ground vehicle crash performance and user acceptability has not been fully tested and evaluated, these systems may have potential for improving the crash survivability of workers in ambulance compartments.
REFERENCES
- FHWA [2000]. Manual on Uniform Traffic Control Devices Millennium Edition. Washington D.C: U.S. Department of Transportation, Federal Highway Administration.
- National Transportation Safety Board Safety Recommendation, H-01-06 through -08. Washington D.C: National Transportation Safety Board, May 2001.
- Byrnes M and Associates [2004]. How to Prepare for the CDL Commercial Drivers License Truck Driver’s Test, 2nd Edition. Hauppauge, NY: Barron’s Educational Series, Inc.
- Spival M [1998]. Buckle up! Kicker vest attendant restraint system protects providers. Emergency Medical Services, 27(11):47-49.
- CDC [2003]. Ambulance Crash-Related Injuries Among Emergency Medical Services Workers – United States, 1991 – 2002. Morbidity and Mortality Weekly Report, Vol. 52, No. 8: 154-156.
- Becker LR, Zaloshnja E, Levick N, LI G, Miller TR [2003]. Relative Risk of Injury and Death in Ambulances and Other Emergency Vehicles. Accident Analysis and Prevention 35: 941-948.
INVESTIGATOR INFORMATION
This incident was investigated by Nancy T. Romano, Safety and Occupational Health Specialist and Paul Moore, Safety Engineer, NIOSH, Division of Safety Research, Surveillance and Field Investigations Branch
Diagrams AND Photographs
|
|
|

|

|

|
|
Photo 4. Attendant's seat after crash; note intrusion of drive shaft into compartment |
This page was last updated on 06/02/05.
- Page last reviewed: November 18, 2015
- Page last updated: October 15, 2014
- Content source:
- National Institute for Occupational Safety and Health Division of Safety Research