


Excavation Worker Killed by Flying Rigging When Hook Fails
 ShareCompartir
ShareCompartir
Oregon Case Report: 05OR024
August 4, 2006
Summary
On June 10, 2005, a 40-year-old pipelayer was struck in the head by the flying rigging of a towline that failed at an excavation site, and died 2 days later. During installation of a sewer pipeline, a hydraulic excavator, commonly called a track-hoe, pulled a 14,000 lb. steel trench shield forward inside a 14.5 ft trench, using a wire rope and hook system. The pipelayer was standing inside the shield while it was being moved. A hook attached to the track-hoe failed, causing the rigging under tension to snap loose, fly into the trench shield, and hit the pipelayer on the back of his hard hat. The victim was air evacuated to a hospital, where he later died.
 |
The track-hoe involved in this incident was pulling a trench shield forward in a trench for a sewer system when a hook failed and the rigging snapped loose. |
Recommendations
- Hooks and other rigging fixtures should be selected and used properly to prevent loading beyond their structural capacity.
- In a towing or lifting operation, workers should be removed from the hazard area or guarded from the reach of the rigging in the event of failure.
- An excavation site must be inspected daily by a competent person to detect and correct hazards, particularly those related to expected loads on equipment.
- Employers are responsible for ensuring (a) compliance with all safety rules, (b) that equipment is maintained and used according to the manufacturer's instructions, and (c) that workers are properly trained to operate equipment safely.
Introduction
On Friday, June 10, 2005, a 40-year-old pipelayer was fatally injured when a hook on a quick coupler in a rigging system under heavy tension failed, causing the rigging to suddenly snap loose and strike the pipelayer on the back of his hard hat. OR-FACE was informed of the incident on June 12 by OR-OSHA. The employer did not respond to OR-FACE requests for an interview. This report is based on information from Oregon OSHA, Medical Examiner, and media reports.
The employer was a union construction contractor, specializing in underground utility installation since 1947. At the time of the incident, the contractor had 60 workers. A subsidiary of the firm, doing business as a nonunion employer with an additional 35 workers, provided office support and equipment maintenance to the main contractor. No information was available concerning the work experience of the pipelayer.
According to the OSHA inspection, the employer had a safety committee, comprised of management employees, which met monthly. The safety committee, however, was not trained in hazard identification or accident investigation techniques, and did not perform regular site inspections.
An engineering firm examined the equipment in this incident and determined that the unintentional release was caused by misuse of the hook assembly. Supervisors and workers using and maintaining the equipment were unaware of the manufacturer’s written operating and safety requirements for the hook assembly on the arm of the track-hoe.
Investigation
The work being performed at the time of the incident was installation of an underground sewer pipeline for a new residential subdivision project in an Oregon metropolitan area. A 14.5 ft. deep trench had been cut in hard soil at the construction site. A 14,000 lb steel trench shield was placed inside the trench to prevent collapse while work was conducted. The crew was in the process of moving the trench shield forward inside the trench when the incident occurred.
The trench shield was 20 ft long, with a bottom box 8 ft high, and a fitted top box another 6 ft high. The shield was being pulled forward up a 5% grade to a new position inside the trench by a hydraulic excavator, commonly called a track-hoe. The pipelayer remained in the shield while it was being moved, according to the company’s standard practice. His task was to protect the newly laid pipe from being crushed by the moving shield. The access ladder was removed from the trench before the shield was moved, in order to prevent damage to the ladder.
 |
Latched hook welded onto the quick-coupler to replace the original closed “lifting eye” supplied by the manufacturer. |
The rigging used for towing the trench shield consisted of a wire-rope sling with two sections, each with a J-hook and shackle assembly on one end to attach to the load. On the other end, the cables were connected to a single steel ring, with each end doubled back and fastened to its cable with a metal sleeve.
The steel ring connecting the two cables was attached to a J-hook on the arm of the track-hoe. The J-hook was shackled to a latched Gunnebo Johnson Model UKN10 hook that was welded to a Hendrix Quick Coupler attachment on the arm of the track-hoe. A quick coupler allows the track-hoe operator to quickly attach or detach the bucket. The latched UKN10 hook was not part of the original equipment.
The Hendrix Quick Coupler comes from the manufacturer equipped with a closed lifting eye, which the employer removed and replaced with the latched hook to allow an easier rigging setup. Manufacturer safety instructions warn that the coupler and components should not be modified. In addition, the advantage of quicker setup is not clear, because the J-hook and shackle attached to the quick coupler always remained on the arm of the track-hoe, even while digging.
 |
The hook and shackle attached to the track-hoe, like the one shown here (without the cable), snapped loose when the rigging failed and struck the pipelayer. |
 |
| Part of the latch remained attached to the hook welded on the Hendrix Quick Coupler on the arm of the track-hoe. |
A few weeks prior to the incident, the construction crew replaced the latched hook on the quick coupler, because the spring and latch mechanism was plugged with clay and would not stay closed, which allowed the J-hook and shackle to fall off. A new UKN10 latched hook was welded to the quick coupler, but the latch problem recurred. A week later, the maintenance department came to the job site and tack-welded shut the latch on the UKN10 hook, making it a closed ring.
While towing the trench shield on the day of the incident, the latched UKN10 hook on the quick coupler failed. The weight of the load was concentrated on the latch mechanism instead of the working part of the hook, resulting in the hook tip bending outward and releasing the rigging. The J-hook and shackle attached to the coupler flew off, disengaged from the sling, and struck the pipelayer in the trench shield on the back of his hard hat. The hook and shackle weighed 32 pounds.
Coworkers immediately called 911 and placed the ladder back into the trench shield to allow rescue workers to reach the pipelayer. The victim was evacuated by helicopter to the hospital, where he died 2 days later of severe head trauma.
Cause of Death
Head injury with skull fracture and hemorrhage.
Recommendations/Discussion
Recommendation #1: Hooks and other rigging fixtures should be selected and used properly to prevent loading beyond their structural capacity.
Employers and workers need to know and follow safety instructions supplied by equipment manufacturers. In this instance, the closed lifting eye on the Hendrix Quick Coupler attachment should not have been replaced. The manufacturer’s lifting eye was closed and circular in shape, maximizing its ability to withstand lifting and pulling forces from any direction, vertical or horizontal. The latched Gunnebo Johnson Model UKN10 hook that was welded to the quick coupler to replace the original lifting eye was designed for vertical lifting. When using the track-hoe to pull the trench shield, the load was mostly horizontal and the force was concentrated at the tip and latch of the hook, which were incapable of carrying the load.
Recommendation #2. In a towing or lifting operation, workers should be removed from the hazard area or guarded from the reach of the rigging in the event of failure.
Workers should move beyond the potential reach of whipping cables or flying rigging during a towing or lifting operation. If a worker must remain in the hazard area, then other safeguards must be implemented.
Safety regulations for excavation sites include a provision that prohibits workers from being inside a trench shield during movement; but only when being “installed, removed, or moved vertically” (29 CFR 1926.652(g)(1)(iv)). Horizontal movement was specifically excluded from the rule to accommodate the kind of work activity observed in this incident. In this case, a metal-plate guard on the nose of the trench shield could have protected the worker during the towing operation.
Another safeguard involves the use of a secondary connection through a bridal or safety line attached near each end of a tow line, connected to the towing equipment on one end, and the load on the other. The bridal remains slack during towing (Figure 1).
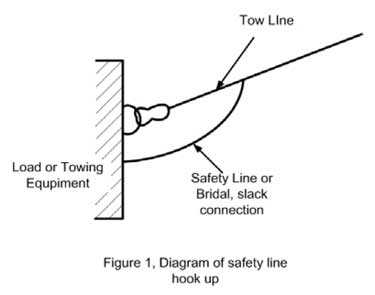 |
Figure 1. Diagram of safety line hook up. |
In this incident, the J-hook attached to the arm of the track-hoe disengaged from both the arm of the track-hoe and the tow line, making it a completely independent missile that could have injured workers well beyond the hazard area designated by the reach of the cables. With the original lifting eye on the Hendrix Quick Coupler, the attached hook and shackle would have been very unlikely to break free. In cases of less certainty, such as this one, the use of a latched hook instead of an open J-hook could keep the hook attached to the wire sling and reduce its range of flight in the event of failure.
Recommendation #3. An excavation site must be inspected daily by a competent person to detect and correct hazards, particularly those related to expected loads on equipment.
Oregon rules for excavation sites require daily inspection of protective systems and operational hazards by a competent person (29 CFR 1926.651(i)(2)(k)). This incident emphasizes the importance of inspecting daily the condition of rigging, cables, and anchor points for lifting and towing operations.
Recommendation #4. Employers are responsible for ensuring (a) compliance with all safety rules, (b) that equipment is maintained and used according to the manufacturer's instructions, and (c) that workers are properly trained to operate equipment safely.
State safety standards address known hazards in the workplace, and employers are responsible to understand and implement the standards to prevent worker injuries. Employers are also responsible to ensure that equipment is maintained and used according to the manufacturer’s specifications and recommendations. Manufacturing instructions for the coupler used in this incident warns users to read the operating manual before attempting to install, operate, or maintain the coupler, and that failure to comply may result in injury or death, and damage to the coupler. Specifications for rigging equipment apply to all lines, hooks, and rigging assembly. Operator and maintenance personnel training should include the equipment manufacturer’s written specifications, operating instructions, limitations, and recommendations for use.
A company safety committee needs to actively pursue safety in the workplace. Safety committee members should be trained in and conduct hazard inspections appropriate to their industry. Work site inspections should be conducted at least quarterly. Committee members should also be trained in accident investigation techniques, in order to detect and correct hazards in a specific work setting.
References
- Gunnebo Chain and Lifting. (n.d.). Universal weld-on hook type UKN. Working load limits available online: http://www.eastwood-dickinson.co.uk/images/gunnebo/product_spec_pdfs
/g8/universal_weld_on_type_ukn.pdf (Link no longer valid) - Hendrix Manufacturing Company. (2003). Information and operational manual for Hendrix Quick Coupler, online: http://www.hendrixmfg.com/_Quick_Coupler_.php (Link no longer valid 3/31/2009)
- Oregon OSHA. (2003). Excavation safety. Available online: http://www.cbs.state.or.us/external/osha/educate/materials/Excavation-Safety-320/1-320i.pdf (Link updated 3/26/2013)
Oregon FACE Program
To contact Oregon State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site. Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.
CROET at OHSU performs OR-FACE investigations through a cooperative agreement with the National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research. The goal of these evaluations is to prevent fatal work injuries in the future by studying the work environment, the worker, the task, the tools, the fatal energy exchange, and the role of management in controlling how these factors interact.
Oregon FACE reports are for information, research, or occupational injury control only. Safety and health practices may have changed since the investigation was conducted and the report was completed. Persons needing regulatory compliance information should consult the appropriate regulatory agency.
- Page last reviewed: November 18, 2015
- Page last updated: October 15, 2014
- Content source:
- National Institute for Occupational Safety and Health Division of Safety Research