


Waste Disposal Worker Was Crushed Between A Waste Disposal Truck and A Dumpster
 ShareCompartir
ShareCompartir

OKFACE Report #03-OK-016-01
SUMMARY
A 45-year old waste disposal worker died on March 24, 2003, from injuries he received when he was crushed between a commercial waste disposal container (dumpster) and the rear-loading waste disposal truck he was operating. Safety latches were not used to secure the dumpster to the truck, and when it was lifted, the dumpster swung around and pinned the victim between the dumpster and the truck. Oklahoma Fatality Assessment and Control Evaluation (OKFACE) investigators concluded that to prevent similar occurrences, employers should:
- Ensure that all waste disposal truck operators attach disposal containers in the proper manner.
- Ensure that continuous training and monitoring for compliance is conducted for all high-risk tasks.
- Ensure that all employees follow written policies and procedures for use of personal protective equipment.
INTRODUCTION
A 45-year old waste disposal worker died on March 24, 2003, from injuries received when he was crushed between a 6-yard commercial dumpster with an empty weight of 970 lbs., and the side of the rear-loading waste disposal truck on which he was the operator. The decedent had been employed as a driver by the waste disposal company for 5½ years and had one year previous experience in the same operation. When he was hired, he had an orientation in the office, rode with an experienced driver for at least 30 days, and then was observed weekly for at least 30 days. He had been picking up at this site for 6 months. The company had been in business for approximately 13 years, and had been picking up at this site for 7 years prior to the incident. OKFACE investigators reviewed the death certificate, the Medical Examiner's report, the OSHA investigation, and newspaper articles on the incident. While conducting the investigation, OKFACE investigators interviewed three employees of the company, including the safety manager who investigated the incident, and the investigating law enforcement officer.
The victim was attempting to empty a 6-yard commercial dumpster into the rear loading waste disposal truck on which he was the operator. The normal procedure for emptying the dumpster involved the operator backing the truck up to the dumpster and attaching a wench cable-lifting hoist to the far end of the dumpster. The operator must also lock the two safety latches (one on each side) on the dumpster’s trunnion bar to stabilize the dumpster as it is lifted and tilted forward (Figure 1).
 |
| Figure 1. Rear of waste disposal truck |
Both locks must be used to properly secure the dumpster to the truck. When the wench cable is engaged, it causes the dumpster to pivot up on the trunnion bars, dumping the contents into the back of the waste disposal truck.
The employer had approximately 70 employees at the time of the incident and had a substantial safety program in place. The program included providing all truck operators with classroom safety training, monthly on-the-job observations and training, and written policies and procedures, including the manufacturer’s safety procedures for operating the equipment. The company also had a strong disciplinary policy for noncompliance with safety measures. The employer observed each truck operator at least once a month on their disposal pick-up route, and the employer maintained records of all employee training and observations completed. The decedent had completed safety training and had received information on incidents in which the safety latches were not engaged and dumpsters swung out. This hazard was also addressed at a safety meeting two months prior to the incident.
INVESTIGATION
At the time of the incident, the conditions were dark and dry. After reporting to work at 3:30 a.m. on the day of the incident, the decedent traveled to the municipality to start his regularly scheduled disposal route. The victim was working alone, as was routine procedure. The truck was approximately one year old and was in excellent condition. At approximately 4:30 a.m. at the second stop for the day, the decedent was attempting to empty a 6-yard dumpster. He was wearing gloves as required, but the required hard hat and safety vest were in the cab of the truck. He backed his truck up to the dumpster so as to position it for lifting and connected the wench cable to the far end of the dumpster. Evidence at the scene indicated that the safety latches were not locked on the dumpster’s trunnion bar. The victim proceeded to engage the wench cable, lifting the far end of the dumpster.
During the lifting procedure, the suspended dumpster dislodged and swung around to the side of the truck where the decedent was standing to operate the controls. The dumpster pinned the victim against the right side of the truck and the controls (Figures 2 and 3).
 | 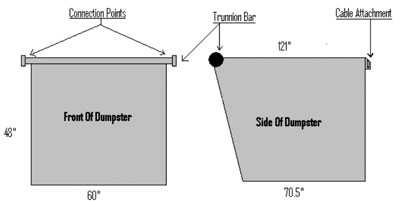 |
Figure 2. Truck with dumpster on side | Figure 3. Diagram of the Dumpster |
Warning signage was posted on the vehicle in all locations of danger, including one directly relating to this type of hazard, positioned where the victim was found (Figure 4).
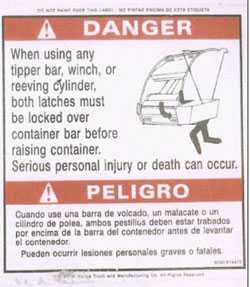 |
Figure 4. Signage located on side of waste disposal truck |
An employee of the company where the dumpster was located noticed the disposal truck on the south side of the building when he arrived at work at approximately 6:50 a.m. The employee stated he had thought that to be unusual since the trash disposal truck was usually not there by the time he arrived at work. He entered the parking lot, walked toward the disposal truck, and observed that the truck was running and the dumpster was against the right side of the truck hanging from a cable.
Upon checking closer, the employee noticed that a man was pinned between the truck and the dumpster. He called out to the victim and did not receive a response. The employee immediately called emergency medical services and then returned to check the victim for responsiveness. The victim was unresponsive and cold to the touch; he was removed from the scene and taken to a funeral home.
CAUSE OF DEATH
The Medical Examiner listed the immediate cause of death as a crushed head and neck.
RECOMMENDATIONS
Recommendation #1: Employers should ensure that all waste disposal truck operators attach disposal containers in the proper manner.
Discussion: Employees should be made aware of the mandatory procedure of using the safety latches to secure the dumpster’s trunnion bar to the truck. In this case, safety training had been completed and documented. Training should include information on the potential consequences of lifting a dumpster if the safety latches are not engaged. The manufacturer’s signage on the side of the truck, located by the controls, depicts what could happen if the dumpster is not attached properly. Wire hoisting cables should also be inspected regularly to ensure that they are in good condition. A Safety and Health Information Bulletin, Crushing Hazards Associated with Dumpsters and Rear-loading Trash Trucks, is available on the Occupational Safety and Health Administration website https://www.osha.gov/dts/shib/shib120903.html.
Recommendation #2: Employers should ensure that continuous training and monitoring for compliance is conducted for all high-risk tasks.
Discussion: The employer should conduct scheduled retraining with employees who are involved in high hazard operations. This retraining could include random/surprise monitoring as well as regularly scheduled training. The employer should also develop a compliance enforcement policy, which works in conjunction with their disciplinary policy and could also include an incentive plan for safety compliance.
Recommendation #3: Employers should ensure that all employees follow written policies and procedures for use of personal protective equipment.
Discussion: The employer should ensure that training on the written procedures and policies for the use of personal protective equipment is completed before any employee is assigned to a job which requires personal protective equipment use. The company should keep all of the training documentation on file and a monitoring system should be developed and utilized to assure compliance with manufacture's recommendations and OSHA CFR 1910 standards for personal protective equipment.
REFERENCES
- NIOSH Publication No. 97-11- Preventing Worker Injuries and Deaths From Moving Refuse Collection Vehicles
- CFR 1910.135 & CFR 1926.951 - Head Protection
- CFR 1910.138 & CFR 1926.951 - Hand Protection
- CFR 1910.132, .252 Protective Clothing
- ANSI Z245.1 - 1992 Mobile Refuse Collection and Compaction Equipment - safety requirements
The Oklahoma Fatality Assessment and Control Evaluation (OKFACE) is an occupational fatality surveillance project to determine the epidemiology of all fatal work-related injuries and identify and recommend prevention strategies. FACE is a research program of the National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research.
These fatality investigations serve to prevent fatal work-related injuries in the future by studying the work environment, the worker, the task the worker was performing, the tools the worker was using, the energy exchange resulting in injury, and the role of management in controlling how these factors interact.
To contact Oklahoma State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE website. Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.
Back to NIOSH FACE Web
- Page last reviewed: November 18, 2015
- Page last updated: October 15, 2014
- Content source:
- National Institute for Occupational Safety and Health Division of Safety Research