


Master Plumber Dies When Trench Collapses
 ShareCompartir
ShareCompartir
KY FACE #03KY072
Date of Incident: July 29, 2003
Report Release Date: May 27, 2004
Summary
On July 29, 2003, a 35-year-old, male master plumber died when an unshorn trench collapsed. Two employees from the contracting company were speaking with him at the time from the side of the trench. He had searched and diagnosed a water line leak when the walls of the trench collapsed. The plumber was employed by a plumbing company contracted by a commercial establishment to locate and repair a water leak. He died at the scene from asphyxia due to chest compression.
To prevent future occurrences of similar incidents, the following recommendations have been made:
- Employers should train employees on safe work practices and how to recognize and avoid unsafe work conditions.
- Employers should train employees working in excavations on the use of appropriate protective equipment.
- Employers should ensure appropriate training and refresher procedures for all employees handling seldom used equipment.
Background
A master plumber with 15 years of experience had been employed approximately 8 months by the commercial division of a plumbing company which had been in operation for 50 years. He was also the foreman on job sites. Ten years ago, the company separated into 3 divisions to provide plumbing services for residential, commercial and industrial. The company had locations in two cities. The decedent worked for the commercial division in one city which employed 2 master plumbers, 2 licensed plumbers, 2 apprentices, 1 drain cleaner and 4 laborers. The 2 apprentices floated from job site to job site on an as-needed basis.
Every Monday an owner/manager held tool box talks at the division where the decedent worked. Tool box talks were held in the other city by the owner/manager each Thursday. Monday’s July 21, tool box talk was on excavating and shoring. The company’s safety policy dictated that any excavation three feet deep or more required two employees to be on site. Typically, the jobs the commercial division contracted did not require trench work over three feet. When jobs required trench work four feet or over, it was company policy to rent shoring equipment such as trench boxes. The plumbing company owned a ¾ size backhoe to dig ditches and trenches; however, if the job required it, the plumbing company would rent a larger backhoe.
Investigation
On July 30, 2003, the Kentucky Fatality Assessment Control & Evaluation program became aware of an occupational fatality involving a master plumber in a collapsed trench. A site visit was made that same day. Photographs were taken at the scene and contact was made with the company that employed the decedent. The coroner was interviewed by phone as was the Kentucky Occupational Safety and Health compliance officer. A company representative was interviewed in August.
On July 14, 2003, a plumbing company was contracted to locate and repair a water leak which had been leaking for two months at a rate of one gallon per second. As each phase of the job was completed, the cost of the next phase was to be negotiated and agreed upon before work continued.
The first phase was to locate the leak. Upon inspection of the interior plumbing lines, it was determined the leak was in the exterior water line between the water meter and the building. Approval to have a leak detection company subcontracted to inject an inert gas into the exterior water lines was submitted by the contractor and approval by the company was granted. After two days of injecting gas into the water lines, the subcontractor determined there were two leaks, approximately 40 feet apart from each other. Leak No. 1 was located away from the building, closer to the water meter; Leak No. 2 was between Leak No. 1 and the building.
The company’s backhoe was brought to the work site to excavate the pavement, grading and soil down to the water line where Leak No. 1 was thought to be located. A trench box was rented and delivered to the site. The company’s backhoe was not large enough to handle the trench box and a larger backhoe was rented and delivered to the job site to help maneuver the trench box in and out of the hole. A storm sewer ran parallel to the building while the water lines ran perpendicular from the building to the street and crossed the storm sewer.
Work to uncover and repair Leak No. 1 commenced with the master plumber and an apprentice excavating and shoveling a hole eight feet deep. It is not known if the trench box was used in this eight foot hole. By the end of the workday on Friday, July 25, the first hole had been dug, and repair of Leak No. 1 had been completed and the hole was partially filled with rock to a depth of four feet.
The work site was secured at the end of each work day by parking heavy equipment near the trench and stringing caution tape around the perimeter of the excavated area. This provided a warning barrier to keep people away from the excavation.
On Monday, July 28, the plumbing company negotiated another phase of the repair to begin on Tuesday, July 29. Work commenced on that day and a second storm sewer was discovered. It was decided by the company and contractor not to locate and repair Leak No. 2 instead, the repair would entail encapsulating the 2 inch water line in a four inch pipe and filling the surrounding space with concrete. This new line would run from Leak no. 1 and tie straight into the building, bypassing Leak No. 2. This made the repair of leak no. 2 unnecessary.
On July 29, the decedent was working alone on Leak No. 2. He used the backhoe to excavate until he found the second leak. It is unknown why he was repairing Leak No. 2. The trench was 8 feet deep and not shored. As the decedent stood in the trench and explained to two employees from the contracting company that he had found the second leak, the trench collapsed, burying him. Emergency services and the victim’s employer were called. It took emergency services approximately 7 hours to excavate the scene and remove the decedent. The coroner was summoned and pronounced the victim dead at the scene.
Cause of Death
The coroner’s report lists the cause of death as due to asphyxia from chest compression.
Recommendations/Discussion
Recommendation No. 1: Employers should train employees on safe work practices and how to
recognize and avoid unsafe work conditions.
Discussion: The Occupational Safety and Health Standard CFR 1926.21(b)(2) states the employer is responsible for training each employee on hazard recognition and avoidance thereof. According to a company official, it was unusual for employees to work in trench conditions 5 feet or above, which would require shoring. It is unclear if the decedent understood the dangers of working in a trench 5 feet deep or more and the importance of taking appropriate safety precautions when working in such situations.
Recommendation No. 2: Employers should train employees working in excavations on use of
appropriate protective equipment.
Discussion: Employers are required by OSHA Standard CFR 1926.652(a)(1) to protect employees from cave-ins while performing excavation work. This regulation also stipulates configurations for sloping sides of trenches and appropriate materials to be used in shoring walls of excavation sites. Any trench over 5 feet or more in depth must have an adequate protection system. Shoring equipment had been delivered to the site, but it is unclear if it was used in the first excavation. It is clear that the shoring equipment on site was not used in the second excavation, which collapsed.
Recommendation No. 3: Employers should ensure appropriate training and refresher procedures
for all employees handling seldom used equipment.
Discussion: The employee involved in this incident did not use shoring equipment very often. It is unclear if he understood how to properly install and use the shoring equipment that was delivered to the site. It is possible that the shoring equipment was not suitable for either of the excavations. Other types of shoring equipment were available for rent. If the decedent had been properly trained in the use of shoring equipment, he could have made an educated decision to use more appropriate materials to brace the sides of the excavations.
References
- Occupational Safety and Health Standard CFR 1926.21(b)(2)
- Occupational Safety and Health Standard CFR 1926.652(a)(1)
- KY FACE Report 03KY056
Acknowledgements
Company Officials
Kentucky Occupational Safety & Health Compliance Officer
Illustrations
 | |
Excavation site where waterline was being repaired. | |
 | |
Street Diagram | |
 | |
| Photograph of Leak No. 1 excavation. Excavation for Leak No. 2 where incident occurred was immediately filled in by the plumbing contractor after decedent had been removed by emergency personnel. This photo was taken the day after the incident. | |
 | 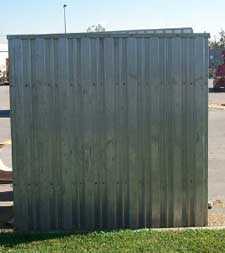 |
| Trench box similar to one available at the work site. The metal arms expand and contract to adjust the size of the box as needed in the excavation. A backhoe was on site to maneuver the box into the hole. | |
The Kentucky Fatality Assessment & Control Evaluation Program (FACE) is funded by a grant from the Centers for Disease Control and the National Institute of Safety and Health. FACE's purpose is to aid in the research and prevention of occupational fatalities by evaluating events leading to, during, and after a work related fatality. Recommendations are made to aid employers and employees to have a safer work environment. The current foci of the program are occupational fatalities involving: construction, machinery, immigrant workers (particularly Hispanics) or youths.
To contact Kentucky State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.
 |
Back to NIOSH FACE Web
- Page last reviewed: November 18, 2015
- Page last updated: October 15, 2014
- Content source:
- National Institute for Occupational Safety and Health Division of Safety Research