


Emergency Medical Technician Dies In Ambulance Crash - New York
 ShareCompartir
ShareCompartir
NIOSH In-house FACE Report 2001-12
February 13, 2004
Summary
On July 13, 2001, a 27-year-old female Emergency Medical Technician (EMT) [the victim] died when the ambulance she was working in struck a support column for an elevated train track. (Photo 1) The victim had been riding unrestrained in the patient compartment while attending to a patient during a non-emergency medical transport. The ambulance was traveling along a two-lane city street when it drifted across the roadway through an oncoming traffic lane and struck the support column. During the collision, the EMT/driver who was also riding unrestrained, sustained minor injuries from contact with the dashboard and deployed air bag. The victim and the patient struck the front of the patient compartment. The EMT/driver and the patient were transported by ambulances to a hospital where they were admitted. The victim was transported by ambulance to a hospital where she was pronounced dead.
NIOSH investigators concluded that, to help prevent similar occurrences, employers should
- ensure that emergency service workers use the patient compartment vehicle occupant restraints whenever possible
- ensure that patient cots are equipped with upper body safety restraints for use during emergency and non-emergency transports
- ensure that drivers and front-seat passengers of emergency service vehicles use the vehicle occupant restraints that are provided.
Ambulance manufacturers and emergency services should
- evaluate and develop occupant protection systems designed to increase the crash survivability of EMS workers in ambulance patient compartments while still providing the necessary mobility to provide patient care during transport.
Introduction
On July 13, 2001, a 27-year-old female EMT (the victim) died when the ambulance she was working in drifted across the road and struck a support column for an elevated train track. On July 18, 2001, the Division of Safety Research (DSR) learned of the incident via the web site http://www.firehouse.com. On August 8, 2001, two Safety and Occupational Health Specialists investigated this incident. Interviews were conducted with the ambulance service owner, and the ambulance was examined and photographed. The city police report, along with case information from the National Highway Traffic Safety Administration (NHTSA), National Automotive Sampling System (NASS) were reviewed.
The employer was an independent ambulance service which had been in business for 45 years. The service had 120 employees, including 85 EMTs and 16 paramedics. The employer estimated that approximately 18% of their ambulance responses were emergency calls, while the rest were to transport patients to and from the hospital or their personal residence.
Equipment. The 1996 Type II* ambulance involved in this incident was previously owned and had been purchased by the ambulance service in 1999. The ambulance had a gross vehicle weight rating (GVWR) of 7,776 lbs. Weight at the time of incident is unknown. There were no known defects that would affect the vehicle’s performance.
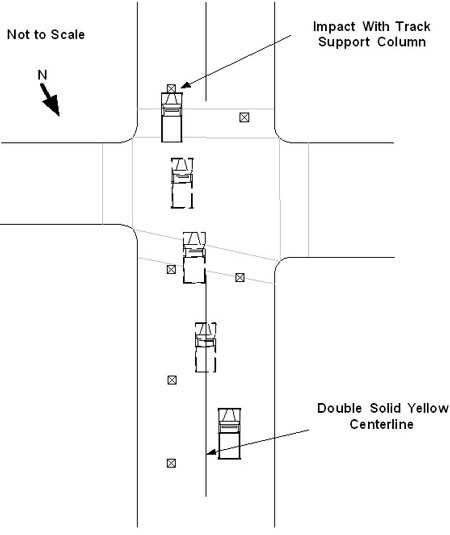
Street Conditions/Weather. The two-lane street on which the ambulance was traveling was marked with a double solid yellow center line. The elevated train track was supported by H-section steel columns approximately 14 by 14 inches set on concrete footings in the crash site. The street has a posted speed limit of 30 mph. The weather on the day of the incident was cloudy, and the street was dry.
Policies/Training. The employer had written policies and procedures that included a mission statement, rules and guidelines for ambulance drivers, and daily vehicle maintenance checks. The company requires each driver to perform a pre-shift vehicle inspection and complete an inspection sheet on the assigned emergency vehicle. In addition, each vehicle receives preventive maintenance service every 3,000 miles by a contracted maintenance facility. Company policy requires that while the ambulance is in motion all occupants must wear the vehicle’s occupant restraints (seat belts).
 |
|
Photo 2. Northern approach to crash site showing track support columns (source, National Automotive Sampling System)
|
The EMT/driver had been with the company for approximately 14 months, 10 of those months as a driver, and had completed a State offered emergency vehicle operators course (EVOC). The victim was a certified EMT also with approximately 14 months of experience with the company. The victim and the EMT/driver were working an 8-hour shift, and they had completed three ambulance responses before this incident.
This was the company’s first workplace fatality.
* Type II ambulances are cargo vans that have been modified to include a patient compartment and a raised fiberglass roof.
Back to Top
Investigation
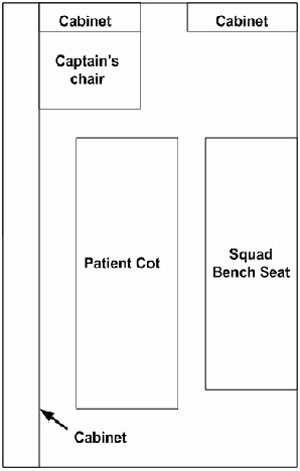
On the day of the incident, the ambulance crew, an EMT/driver and an EMT (the victim), had been assigned to transport a 74-year-old male patient from a hospital to his residence. The crew departed the hospital with the patient at approximately 11:56 am. The patient had been placed on the patient cot, secured with lap-belt type leg and hip restraints and loaded into the ambulance. The ambulance was traveling southbound and without lights and sirens on a two-lane city street. The EMT/driver was unrestrained, while the EMT (victim) was located unrestrained on the left-facing squad bench seat attending the patient. (Figure 1)
At approximately 12:15 pm., 1½ miles from the hospital, the ambulance drifted through the northbound lane toward oncoming traffic and struck the elevated train track support column at an estimated speed of 26 mph. (Photo 2 and Figure 2) The ambulance came to rest with the front against the track support column. (Photo 1) During the collision, the victim continued moving forward, contacted and broke a hand rail located at the forward end of the squad bench and struck the cabinet at the front of the patient compartment. (Photos 3 and 4) The patient was partially ejected from the cot restraints and struck the rear-facing captain’s chair located at the front of the patient compartment before coming to rest partially off the cot. (Photo 5)
At approximately 12:20 pm. the EMT/driver called the office of the ambulance service to report the incident. A witness also called Central Dispatch to report the incident and the city police and several ambulances responded to the incident. Emergency medical service (EMS) personnel arrived on the scene, and found the EMT/driver standing outside of the ambulance. After EMS personnel assessed the scene, the EMT/driver and the patient were transported by ambulance to a hospital where they were both admitted. The EMT/driver sustained minor injuries from contact with the vehicle’s dash and the steering wheel mounted air bag as it inflated. He was discharged from the hospital 3 days after the incident. The patient contacted the captain’s chair at the bulkhead between the patient compartment and the driver’s compartment, sustaining spinal and rib-cage fractures and head injuries. He was discharged from the hospital 12 days later. The victim sustained spinal and head injuries during the incident. She was transported by an ambulance to a hospital where she was pronounced dead at 1:18 pm.
 |
|
Photo 3. Victim contacted and broke a handrail at forward end of squad bench (source, National Automotive Sampling System)
|
A conclusive determination as to why the ambulance veered left across traffic and struck the support column could not be made. However, the NASS case file for this incident indicated that no avoidance maneuvers had been attempted and under the category for distraction, it listed “inattentive or distracted, sleepy or fell asleep.”1 Also, witnesses interviewed indicated that the driver had no recollection of the crash.
Back to Top
Cause of Death
The cause of death, reported in the NASS report was:
- Thoracic spine cord laceration; complete cord syndrome with dislocation;
- Lung contusion bilateral with or without hemo-pneumothorax;
- Cerebellum subarachnoid hemorrhage.
These injuries were attributed to direct contact with the bulkhead/cabinet separating the patient compartment from the driver’s cab.
 |
|
Photo 4. Victim contacted cabinet at the front of the patient compartment (source, National Automotive Sampling System)
|
Recommendations and Discussion
Recommendation #1: Employers should ensure that emergency service workers use the patient compartment vehicle occupant restraints whenever possible.
Discussion: The patient compartment of the ambulance involved in this incident was configured with four seating locations each equipped with two-point lap belt type restraints. These positions included a rear-facing high-backed captain’s chair and a squad bench with accommodation for three persons. (Figure 1)
The employer’s written policies required that everyone in the ambulance wear restraints while the ambulance was in motion. However, when the squad bench lap belts were examined by the NHTSA NASS researcher, no evidence of usage could be found. Additionally, had a lap belt restraint been used, the EMT would most likely not have impacted against the front bulkhead during the collision. It should be noted that the lap-belt restraint systems commonly used in ambulances may not allow full access to the patient during treatment for all conditions. When properly used, the squad bench lap belts position the occupant against the side wall in such a manner that the EMT may be impeded in moving or bending toward the bench edge to access the patient. If the EMT needs to access the cabinets along the opposite wall, the restraint must be unbuckled to allow the EMT to stand up.
 |
|
Figure 1. Type II Ambulance Patient Compartment
|
Additionally, if it is necessary to perform CPR or other procedure the EMT may need to stand over or kneel near the cot. For these reasons, it may be common practice among EMTs to ride unrestrained, seated on the edge of the squad bench.
However, during non-emergency transport, EMTs could remain seated and restrained in the captain’s chair or alternatively, the EMT could be seated restrained on the squad bench. It is difficult to evaluate the likelihood of injury to the victim had she been using a restraint. However, the patient compartment sustained little damage during the collision and had the victim been seated and restrained on the squad bench, or seated and restrained in the rear-facing captain’s seat she would not have collided with the cabinets near the front bulkhead and her injuries may have been less severe.
Recommendation #2: Employers should ensure that patient cots are equipped with upper body safety restraints for use during emergency and non-emergency transports.
Discussion: During the collision, the patient was partially ejected from the cot and contacted the seat back of the captain’s chair at the front bulkhead. [Photo 5] As previously stated, the patient had been secured to the cot with hip and leg straps. Strap type restraints across a patient’s lower body offer little or no resistance to forward movement induced from frontal collision. Patient restraint systems are available that include shoulder and chest straps in addition to the hip and leg restraints. Had the patient’s restraints included shoulder straps he may not have contacted the captain’s chair seat back.
 |
|
Photo 5. View of patient compartment after the vehicle was recovered from site. Patient contacted seat back at upper location, cot contacted at lower location. Contact indicated by yellow markers (source, National Automotive Sampling System)
|
Recommendation #3: Employers should ensure that drivers and front-seat passengers of emergency service vehicles use the vehicle occupant safety restraints that are provided.
Discussion: At the time of the collision, the EMT/driver was driving unrestrained. The ambulance involved in this incident was equipped with 3-point (lap and shoulder belt) restraints for the driver and front seat passenger. The vehicle was also equipped with a driver’s side airbag. During the collision, the airbag functioned as intended and the driver suffered minor injuries which included a skin laceration from contact with the lower dashboard and abrasions from contact with the deploying airbag. Although the EMT/driver’s injuries were minor, they may have been further minimized if the occupant restraints had been used. Airbags are designed to work as supplemental restraints in conjunction with the lap and shoulder belt. The lap and shoulder belt properly position the occupant so that the protection afforded by the air bag is maximized. Also, air bags deploy during the initial collision of a crash and do not continue to provide protection for subsequent crash collisions.2
Recommendation #4: Ambulance manufacturers and emergency services should evaluate and develop occupant protection systems designed to increase the crash survivability of EMS workers in ambulance patient compartments while still providing the necessary mobility to provide patient care during transport.
Discussion: Currently, ambulance patient compartments are equipped with two-point lap-belt type occupant restraints. As previously noted, proper use of these restraints may preclude EMS worker mobility in the patient compartment and access to the patient for procedures such as CPR. Manufacturers of ambulances and emergency service providers should consider developing and evaluating restraint systems that offer EMS worker mobility while still providing crash protection. Tethered harness type restraints are commonly used by military air crew and similar systems have been used in ground ambulances on a limited scale.3 These systems employ retractor-equipped tethers connected between a harness worn by the worker and strategic locations on the vehicle structure. The retractors provide occupant mobility by allowing the tether strap to roll off of the retractor reel as the wearer moves away from the retractor mount and to roll back on the reel as the wearer moves closer to the attachment point. The retractor automatically locks the reel at predetermined vehicle acceleration levels to limit occupant motion during a crash. The ground vehicle crash performance and user acceptability of these systems has not been fully evaluated. However, they may have potential for improving the crash survivability of workers in ambulance compartments while allowing EMS workers sufficient mobility to provide patient care.
Back to Top
References
- NHTSA [2002]. National Automotive Sampling System (NASS), Case No. 2001-003-051, (Case Id 107003667) Washington D.C.: U. S. Department of Transportation, National Highway Traffic Safety Administration http://www-nrd.nhtsa.dot.gov/departments/nrd-30/ncsa/. (Link no longer valid 9/26/2008)
- NHTSA [2003]. What You Should Know About Air Bags. Washington D.C.: U. S. Department of Transportation, National Highway Traffic Safety Administration, DOT HS 809 575 http://www.nhtsa.gov/people/injury/airbags/airbags03/. (Link Updated 11/17/2011 - no longer available 3/14/2013)
- Spival M. [1998] Buckle up! Kicker vest attendant restraint system protects providers. Emergency Medical Services, 27(11):47-49.
Investigator Information
This incident was investigated by Nancy T. Romano and Kim Cortez, Safety and Occupational Health Specialists and assistance preparing this report was provided by Paul H. Moore, Safety Engineer, NIOSH, Fatality Investigation Team, Surveillance and Field Investigation Branch, Division of Safety Research.
 |
|
Figure 2. Overhead view of incident scene
|
In-house Reports
- Page last reviewed: November 18, 2015
- Page last updated: October 15, 2014
- Content source:
- National Institute for Occupational Safety and Health Division of Safety Research