


Plumber Dies After Being Crushed Between a Tandem Scissors Lift Platform and the I-Beam Frame of a Mobile Home - Tennessee
 ShareCompartir
ShareCompartir
NIOSH In-house FACE Report 2002-04
Summary
On March 11, 2002, a 32-year-old male plumber (the victim) died after being crushed between a tandem scissors lift platform and the I-beam frame of a mobile home. The victim worked as a plumber for a mobile home manufacturing company, and he had crawled under a mobile home that was nearly finished to complete a measurement. A few minutes later the company's tandem scissors lift operator, who had not seen the victim go under the home, began to raise the home to provide adequate space for workers to install wheels on its axles and to install a tongue assembly at the front of the home. The victim was caught between the scissors lift platform and the I-beam when the scissors lift was raised. Coworkers and the victim yelled to the operator to stop. When the lift was lowered, the victim was able to wiggle free. After seeing that the victim had been injured, a supervisor ran to the office and directed the receptionist to call 911. The company safety manager/nurse responded immediately and provided emergency care.
Emergency medical services (EMS) personnel responded within minutes and provided emergency care, then transported the victim by ambulance to a county hospital. Shortly after his arrival at the county hospital, the victim was airlifted to a city hospital where he was pronounced dead later that day.
NIOSH investigators concluded that, to help prevent similar occurrences, employers should
- incorporate specific safe operating procedures for controlling hazardous energy into their scissors lift safety policy, including individually assigned locks and keys to secure energy control devices, and train all workers in the new procedures
- evaluate and upgrade warning systems as needed to maximize their effectiveness
Introduction
On March 11, 2002, a 32-year-old male plumber (the victim) died after being crushed between the platform of a tandem scissors lift and the I-beam frame of a mobile home. On March 11, 2002, officials of the Tennessee Occupational Safety and Health Administration (TOSHA) notified the National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research (DSR), of the incident. On April 9, 2002, a DSR occupational safety and health specialist met with the TOSHA compliance officer to discuss the case and to review information collected and photographs taken during the course of his investigation. Additionally, the DSR safety and health specialist met with company representatives, visited the incident site, and observed the operation of the tandem scissors lift. The official cause of death was obtained from the coroner's report.
The employer was a mobile home manufacturing company that had been in business since 1970. The company had business sites located throughout the United States and employed 7,400 workers nationwide. The incident occurred in one of the company's manufacturing plants that had been in operation for 6 years. This plant employed 178 workers, 140 of whom worked in mobile home assembly jobs.
The employer had a written safety program that included a scissors-lift safety policy. The company had a full-time safety manager on site. The victim had been working for the company for 4 years and had signed documents indicating that he had completed the 1-week orientation provided each worker at the beginning of their employment and had received specific training in the standard operating procedures workers were to follow when working near or under mobile homes. The company's safety committee met on a monthly basis. Toolbox meetings were conducted before work each day. As team leader of a seven-man plumbing crew, the victim conducted toolbox talks and had team members on the company's safety committee give safety updates. This was the plant's first workplace fatality.
Back to Top
Investigation
The mobile home manufacturing plant operated one 8-hour shift per day, 7 a.m. to 3:30 p.m. Three double-wide mobile homes were completed each day (six half-sections). The mobile home assembly was completed in a large warehouse. Building materials needed for each step of the assembly process were stacked on one side of the warehouse. The assembly was done on the other side of the warehouse where a floor-mounted chain conveyor was used to pull each double-wide home through the first seven assembly stations. At Station #7, the double-wide homes were separated into two sections, A and B. Each section was raised separately using several in-floor tandem scissors lifts. After the section was raised, a tongue assembly was installed at the front and wheels were placed on each axle. Up to four tandem in-floor scissors lifts were activated to raise each section depending upon the length of the section. Each lift had a 2,050-pound weight capacity. Once activated, the hydraulic lifts moved at approximately 1 inch per second and could be extended 48 inches. The lift platforms were flush with the floor when fully recessed. Lift platforms measured 24 inches wide by 132 inches long and extended under the width of each section. After each section was completed, a tractor was used to pull the sections to Station #8. At Station #8 the section was inspected, draperies were installed, and the final testing of electrical and plumbing systems was conducted. The sections were then pulled to a storage area until they were distributed to buyers. Sections measured 14 feet wide by 40 to 76 feet long. The section that was being manufactured at the time of the incident was 14 feet wide by 44 feet long.
On the day of the incident, the victim started work at 7 a.m. along with the other production workers. Shortly before 1:40 p.m., a double-wide home was pulled by the chain conveyor system to Station #7 where it was separated into sections A and B. Section A was raised using tandem lifts, and the tongue assembly and wheels were installed. The next step in the work process entailed raising Section B with tandem scissors lifts and installing its wheels and tongue assembly.
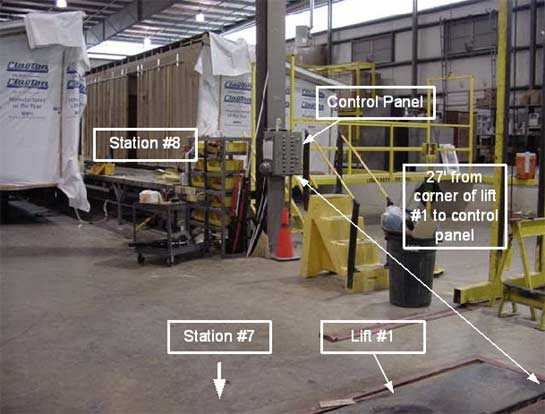
Witness statements indicate that in preparation to raise Section B, the scissors lift operator conducted a visual inspection under and in front of the section as required by the company's scissors lift policy. The company scissors lift safety policy also required workers to place an orange warning cone at the front of the section before entering or climbing underneath. Seeing no worker under the section and seeing no orange warning cone placed at the front of the section, he turned around and walked back to the control panel located approximately 27 feet in front of the section. The lift operator inserted his key into a lock on the control panel and used the key to turn the switch to the "on" position. The switch powered the control panel buttons that were used to operate the hydraulic scissors lifts (Photo 1).
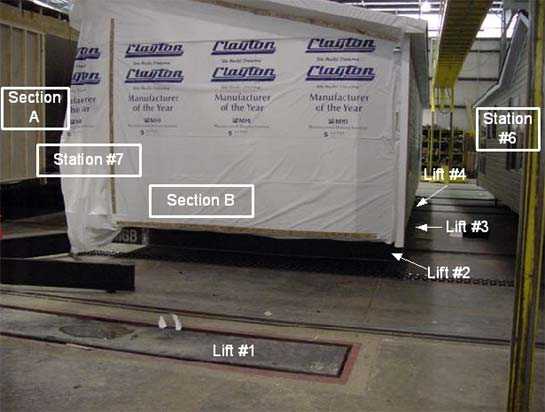
Evidence suggests that at approximately the same time that the lift operator was making preparations for the lift, the victim had walked down the right side of Section B without the lift operator seeing him. He crawled under the section at the location of tandem scissors lift #3 to perform a job that normally takes approximately 30 to 60 seconds. The job entailed cutting the plastic covering under the section and reaching through to take a pipe measurement for a lavatory drain (this drain is similar to the elbow under a sink). The victim crawled under the home and positioned himself on his back approximately 32 inches in from the side of the section on the platform of tandem scissors lift #3 (Photo 2). He was directly under a 12-inch-wide I-beam in a space that measured approximately 9.5 inches from the surface of the scissors lift platform underneath him to the surface of the I-beam above him (Photo 3). At the same time, two carpet installers carrying a roll of carpet walked alongside Section B at Station #7, saw the victim's legs extending out from under the section, and asked him to pull his feet in so that they could walk past him.
The lift operator meanwhile continued preparations to raise the section. Because the section was 44 feet long, he raised lifts #3 and #4 by pushing buttons that controlled individual lifts. Lifts #1 and #2 were not activated as they were used only for longer sections and would have blocked the area where the hitch assembly was to be attached. A warning bell was wired into the control panel and was designed to sound a warning only when all four tandem lifts were activated at once. Therefore, no warning bell sounded when only lifts #3 and #4 were raised. The victim yelled for the operator to stop when the lift he was lying on began to rise. Carpet workers knew the plumber was under the section and yelled to the operator to lower (recess) the lifts. The operator heard the yells and pushed one button that controls downward motion for lifts #1 through #4. Lifts #3 and #4 recessed while lifts #1 and #2, which had not been raised, remained recessed. Other workers in the area, unaware of the victim's location between the lift and the I-beam, yelled for the operator to raise the lifts. The operator pushed one button that controls upward motion for the lifts and raised lifts #1 through #4. This time the warning bell rang because all four lifts were raised at once. The operator heard more yells and pushed one button to lower lifts #1 through #4.
After the lifts were recessed, the victim managed to wiggle free from his position between the lift and the I-beam. Given that the space between the I-beam above the worker and the in-floor lift platform under the worker was 9.5 inches, the lifts may have moved only several inches up and down each time they were activated.
One witness indicated to the TOSHA compliance officer that he remembered seeing an orange warning cone in front of Section B before the victim went under it. An orange cone was found wedged under the tongue assembly which had been moved to the left after the incident. It could not be determined whether or not the victim had placed this cone in front of the home before crawling under it. According to company representatives, spare cones were kept near the sections for use by employees.
A supervisor, who had been working on the opposite side of Section B, heard the yelling and responded immediately. When he saw that the worker was injured, he ran toward the front office to get help. On his way he met the production manager who in turn told the office receptionist to call 911. The plant safety manager/nurse, who was working in an office in another building, heard the commotion on her company radio and responded immediately. She provided emergency medical care until EMS personnel arrived. EMS personnel responded within minutes, continued emergency care, and transported the victim by ambulance to a county hospital. The victim was airlifted to a city hospital where he was pronounced dead later that day.
Following the incident, the company made extensive revisions to its scissors lift safety policies and procedures.
Back to Top
Cause of Death
The coroner's report indicated that the cause of death was multiple abdominal and chest injuries.
Recommendations/Discussion
Recommendation #1: Employers should incorporate specific safe operating procedures for controlling hazardous energy into their scissors lift safety policy, including individually assigned locks and keys to secure energy control devices, and train all workers in the new procedures.
Discussion: Employers should develop and implement a written hazardous energy control program that protects workers who must work in situations where hazardous energy could be released. The program should include, at a minimum,
- a description of safe work practices
- machine-specific lockout/tagout procedures
- training for all workers in the procedures
- enforcement procedures including disciplinary action for failure to follow them
The lockout/tagout program should require individually assigned lock and keys to secure energy control devices. Lockout/tagout programs should be based on the principle of only one key for each lock the worker controls, meaning
- workers are assigned individual locks operable by only one key for use in securing energy control devices, such as breaker panels
- each worker maintains custody of the key for each of his or her assigned locks
- each lock is labeled with a durable tag or other means that identifies its owner
- when work is performed by more than one worker, each worker applies his or her own lock to the energy-securing device
- all de-energized circuits and systems are clearly labeled with durable tags
- the worker who installs a lock is the one who removes it after all work has been completed
- if work is not complete when the shift changes, workers arriving on shift apply their locks before departing workers remove their locks
Because tags can be easily removed, they are not a substitute for locks. Workers are safest with a program that uses both locks and warning tags to prevent systems from being inadvertently re-energized [NIOSH 1999]. 1 For these procedures to be effective, they must be clearly communicated and fully understood by affected employees and supervisors.
The scissors lift safety procedures should state clearly that whenever possible, work under sections should be postponed until the section has been fitted with wheels and has been moved out of the lift area.
Employers may find the following resources useful in improving their safety programs: NIOSH Alert: Preventing Worker Deaths From Uncontrolled Release of Electrical, Mechanical, and Other Types of Hazardous Energy 1, Code of Federal Regulations 1910.147 The Control of Hazardous Energy (Lockout/Tagout) 2, and Chapter 6: Job Safety Analysis, Accident Prevention Manual. 3
Note: Following the incident, the company made changes in its scissors lift safety policy and in safety procedures workers were to follow when working with or around the scissors lift. A lockable control box power disconnect was installed between the control panel for the scissors lift and the power source. The new procedure requires workers to place their personally assigned lock and tag on the newly installed control box power disconnect before working under a section at Station #7 (the lift station). The new policy includes progressive discipline for any worker that does not follow the new safety procedures.
Recommendation #2: Employers should evaluate and upgrade warning systems as needed to maximize their effectiveness.
Discussion: Properly designed and strategically placed warning alarms and lights can provide workers with advance warning of changing conditions that may affect their safety. At the time of the incident, the control panel for the lift was equipped with an alarm that sounded only when all four lifts were raised or lowered simultaneously but not when lifts were raised independently. Alarms sounded as the lifts moved. Alarms were used to provide a warning to workers in the area of lift movement and should be redesigned to sound whenever even a single lift is activated. A delay should be built into the system to allow workers sufficient time after the alarm sounds to vacate the hazardous area before lift movement.
Additionally, employers should consider installing warning lights, such as strobe lights, in locations where they can alert all affected workers. These warning lights should be synchronized with the lift control panel so that whenever the control panel switch is turned on, the lights flash and provide an additional warning that the lift is operating. Employers should also consider painting the lift platforms with caution stripes to help workers see where the lifts begin and the solid floor ends.
Note: The company reconfigured the control panel for the lifts after the incident. The alarm sounds when the lift operator's key is placed in the switch on the power panel; after a 5-second delay the lift can be activated. As an additional safety precaution, the company painted yellow and black diagonal warning stripes on all in-floor scissors lifts at Station #7. They also installed a strobe light that is activated when the scissors lift switch is turned on to provide a visual alarm to workers under the mobile home that the lift has been activated. The company chose to retain the use of orange cones as an added visual warning that a worker is under the home. These cones are now labeled for each department and all spare cones are placed in storage. Two additional workers are assigned to work as spotters. Along with the lift operator, they visually inspect the area under the section before activating the lifts.
Back to Top
References
- NIOSH [1999]. NIOSH Alert: Preventing worker deaths from uncontrolled release of electrical, mechanical, and other types of hazardous energy. U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No. 99-110.
- Code of Federal Regulations 2001 edition. 29 CFR 1910.147 The control of hazardous energy (lock-out/tagout). U.S. Printing Office, Office of Federal Register, Washington, D.C.
- National Safety Council [1997]. Accident prevention manual. Itasca, Illinois; pp. 134-139.
Investigator Information
This investigation was conducted by Doloris N. Higgins, Safety and Occupational Health Specialist, Fatality Assessment and Control Evaluation Team, Surveillance and Field Investigations Branch, Division of Safety Research.
Photographs
In-house Reports
- Page last reviewed: November 18, 2015
- Page last updated: October 15, 2014
- Content source:
- National Institute for Occupational Safety and Health Division of Safety Research