


Sixteen-Year-Old Produce-Market Worker Dies From Crushing Injuries After Being Caught in a Vertical Downstroke Baler - New York
 ShareCompartir
ShareCompartir
NIOSH In-house FACE Report 2000-19
Summary
A 16-year-old male produce-market worker (the victim) died from crushing injuries after being caught in the vertical downstroke baling machine that he was operating (Figure 1). The victim, working alone in the basement of a small produce market, was crushing cardboard boxes when at some point in the compacting process he was caught by the machine's hydraulic ram. The victim was discovered by an exterminator spraying the basement, who notified the store manager to call police and emergency medical services (EMS).
Subsequent examination by investigators revealed that the safety interlock had been bypassed, allowing the machine to operate with the loading door in the open position. The victim may have reached into the baling chamber during a compression cycle to adjust a tie wire or a liner box and was caught by the ram platen.
NIOSH investigators concluded that, to help prevent similar incidents, employers should:
- ensure that all safety devices on baling machines are functioning correctly and enforce proper operation
- ensure that employees, including management personnel, know and understand the importance of the machine's safety features
- comply with child labor laws which prohibit youth less than 18 years of age from operating or assisting to operate paper balers
- develop and implement a comprehensive employee safety program that includes training in the safe operation of machinery and the importance of the machine's safety devices
Introduction
On July 27, 2000, a 16-year-old male produce-market worker (the victim) died as a result of crushing injuries he sustained from a baling machine used to compress waste cardboard boxes into bales for disposal/recycling. On July 28, 2000, the National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research (DSR), was notified of the incident by the U.S. Department of Labor, Wage and Hour Division, and initiated an investigation. On July 31, 2000, a DSR occupational safety and health specialist conducted a site visit and met with representatives of the Occupational Safety and Health Administration (OSHA), the New York City Police Department, and the market's manager. During the site visit, information was collected regarding the market's safety programs, a tour of the facility was conducted, the baling machine was observed and photographed, and information pertaining to the incident was collected.
The produce market where this incident occurred had been in business at its current location for over 15 years, specializing in fruits and vegetables, gourmet cheeses, and fishes and meats. The market employed approximately 65 workers, working three shifts a day. The majority of the employees worked the day and evening shifts during peak business hours. The third-shift workers, who started at 11:00 p.m., were primarily responsible for restocking shelves and providing janitorial services. At the time of the incident there were eight employees working the third shift. The market had no formal or written safety policies, nor was there a trained safety person on site. The victim had worked for the market for approximately 3 weeks as a general stockboy. This was the market's first workplace fatality.
Back to Top
Investigation
At this market, a large volume of empty cardboard boxes was accumulated from restocking shelves. To manage the boxes, the market installed a small vertical downstroke baling machine to compress the boxes into bales for disposal or recycling.
On the night of the incident, the victim started work at approximately 11:00 p.m. Sometime during his shift, he was instructed to compress and bale waste cardboard boxes using the baler. The baler was located in an isolated area in the basement of the market. At approximately 2:00 a.m., an exterminator setting traps in the basement that night saw the victim and called out a greeting. When he did not get a response from the victim, he walked over to the baler, where the youth was slumped over at the waist and leaning into the loading chamber of the baler. The exterminator saw that the youth had been seriously injured and immediately notified the night manager, who called emergency services and police. When EMS arrived they found that the youth had been fatally injured and waited for the police to arrive and conduct their investigation before removing the body from the site.
The baler involved in this incident was a Harmony Enterprises, Model M36HD, vertical downstroke baler. According to the market's manager, the baler was purchased new approximately 2 years prior to the incident and was installed by the manufacturer. Initial training in the proper operation of the baler was also provided by the manufacturer. After the initial training, the employer was to assume responsibility for training employees. The market had no formal training programs and any training that may have been provided was through watching other employees operating the baler and on-the-job use of the baler.
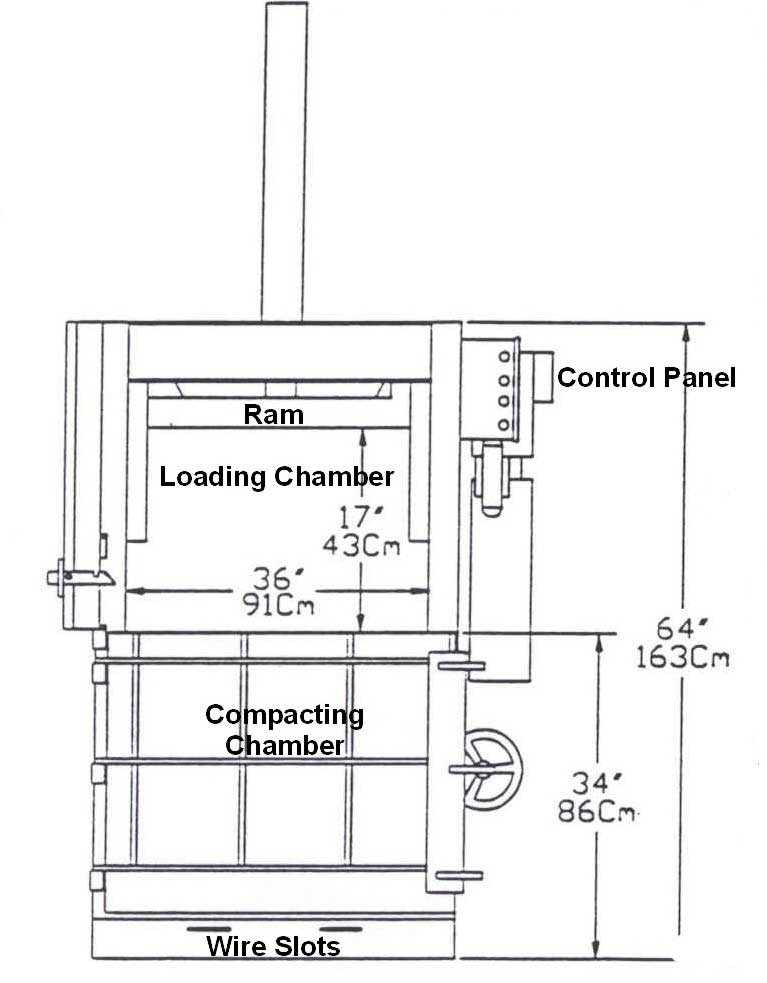
The dimensions of the baler are shown in Figure 2. The baler stands 96 inches high by 32 inches wide and utilizes hydraulic pressure to compress materials. A maximum ram pressure of 41,350 pounds can be generated from the 1½ horsepower electric motor and two stage hydraulic pump. An electrical control panel is mounted on the front, upper right side of the baler. The control panel is equipped with three buttons marked UP, DOWN, and EMERGENCY STOP (Figure 3).
There are two doors on the front of the baler; a lower door provides access to the baling chamber and an upper door is for loading material. The workable area for loading the baler with the upper door open is 17 inches high from the ram to the top of the lower door, by 36 inches wide and 32 inches deep. This baler can produce bales of compressed material measuring 24 inches by 36 inches by 30 inches and weighing up to 250 pounds. The manufacturer provides operating procedures in the baler's users' manual.
According to the manufacturer's instructions, the first step in operating this baler is to thread the twine or wire through the machine for securing the bale after compression. This is done by first pulling the twine up and over the twine guide on the back side of the baler, leaving enough twine lying on the bottom of the compression chamber floor to pull through two slots cut in the front of the baler. Once the twine is secured to the outside, the loading cycle can begin. The operating instructions state that the power should then be disconnected, to prepare the compression chamber by applying paraffin wax to the inside walls of the chamber, before the lower loading door is closed and latched. The next step is to reconnect the power and open the upper loading door. A large flattened box is then placed on the floor of the compression chamber (on top of the twine) to serve as a base for the new bale. Once the baling chamber is full of material to be compressed, the upper loading door is to be closed and the DOWN button depressed, starting the ram on its downward stroke. There is a safety interlock that will not allow the ram to start downwards if the upper loading door is open. Also, if the door is opened during a compression cycle, the safety interlock shuts off power to the motor, stopping the ram. On the return stroke, as the ram reaches the top of the baler, it engages a limit switch that shuts off the motor, completing one compression cycle. One complete compression cycle takes approximately 40 seconds.
In an effort to speed up the process of compressing boxes at this market, workers had defeated the safety interlock on the upper door. A wad of paper had been jammed into the hole that the door pin passed through, to simulate the door being closed. By defeating the interlock, the baler could be operated with the upper loading door open. When the victim was found, it appeared that he had been just starting a new bale. The wire had been threaded through the baling chamber and secured to the outside of the baler and a flattened box was in place in the base of the compaction chamber. He may have leaned over into the compression chamber trying to quickly adjust a tie wire or the base box when he was caught in the ram as it moved downwards.
Back to Top
Cause of Death
The Medical Examiner listed the cause of death as multiple traumatic injuries due to compression by a baler recycling machine.
Recommendations and Discussion
Recommendation #1: Employers should ensure that all safety devices on baling machines are functioning correctly and enforce proper operation.
Discussion: The baling machine involved in the incident was equipped with safety devices in compliance with ANSI Z245.5-1997 standards for Baling Equipment-Safety Requirements. Specifically, the machine was equipped with a loading chamber closure consisting of a door that had a plunger pin welded at the bottom. When the door is closed, the pin passes through a small hole in the frame of the baler and engages a power interlock switch, allowing operating power to the motor and hydraulic pump. When the door is opened, the interlock switch is disengaged, cutting power to the motor and hydraulic pump. In this incident, the interlock power switch was bypassed with a wad of paper jammed into the pin hole to simulate the door pin. By doing so, the baler was allowed to operate with the load chamber door open. If the interlock had been operable, this incident may not have occurred.
Recommendation #2: Employers should ensure that employees, including management personnel, know and understand the importance of the machine's safety features.
Discussion:In this case, the safety interlock on the loading door had been perceived as a hindrance in speeding up the cycle time of the machine. Bypassing the safety interlock was one method of removing this hindrance. However, bypassing these devices increased the potential for exposure to risk of crushing or amputation during operations, and in this case resulted in a fatality. Additionally, a coworker reported that he had injured his hand in the baler during the preceding year when he had reached into the loading chamber during a compression cycle to adjust a cardboard box.
When the safety devices are operating correctly, they pose no hindrance to efficient operation and protect against the inadvertent exposure of persons to the movement of the ram. Additionally, an operating manual for the machine was not available and neither workers nor management had adequate experience or knowledge of this type of equipment, nor did they appear to comprehend the potential for injury.
Recommendation #3: Employers should comply with child labor laws which prohibit youth less than 18 years of age from operating or assisting to operate paper balers.
Discussion: The Fair Labor Standards Act provides a minimum age of 18 years for nonagricultural occupations which the Secretary of Labor "shall find and by order declare" to be particularly hazardous for 16- and 17-year-old persons. The Secretary has issued 17 Hazardous Occupations Orders. Hazardous Occupation Order No. 12 (HO 12) prohibits 16- and 17-year-olds from operating or assisting to operate paper balers or compactors. A limited exemption from this prohibition is allowed by the Compactors and Balers Safety Standard Modernization Act of 1996, Public Law 104-174 which provides that 16- and 17-year-old workers are allowed to only load (place materials in), but not operate or unload materials from, scrap paper balers and cardboard box compactors, provided that the machines meet certain operation and construction standards.
Additionally, employers must post a notice that the machine meets the standards; 16- and 17-year-old workers are allowed to load only; and employees under the age of 18 may not operate or unload the scrap paper baler or compactor. Compliance with the Act can protect adolescent workers from baler and compactor hazards by limiting exposure to moving machine parts, and ensuring that older, more experienced workers are available to detect and correct hazardous work practices. Finally, for workplaces that employ minors, it is important to train all adult employees on what jobs the minors are permitted and prohibited from doing at the work place.
Recommendation #4: Employers should develop and implement a comprehensive employee safety program that includes training in the safe operation of machinery and the importance of the machine's safety devices
Discussion: The operating instructions describe numerous warnings and proper operating procedures to safely operate this baler. The victim and coworkers in this incident apparently lacked the understanding and training necessary to safely operate and maintain this machine. It is recommended that a written safety program be developed that includes provisions for supervisors and workers to be trained and certified in the safe operation of the machines before being allowed to use or maintain the equipment. Periodic re-evaluation should be required to ensure the worker is knowledgeable in operating and safety procedures. Training should include standard operating procedures and safety practices unique to each piece of equipment.
Back to Top
References
- American National Standards Institute, Inc. (1997). American National Standard for Equipment Technology and Operations for Wastes and Recyclable Materials - Baling Equipment - Safety Requirements. ANSI Z245.5
- U.S. Department of Labor. Child Labor Requirements in Nonagricultural Occupations Under the Fair Labor Standards Act, Code of Federal Regulations, Title 29, Section 570.
- Compactors and Balers Safety Standards Modernization Act, Public Law 104-174, August 6, 1996.
Investigator Information
This investigation was conducted by Joseph E. Burkhart, Occupational Safety and Health Specialist, NIOSH Division of Safety Research, Surveillance and Field Investigation Branch, Fatality Assessment and Control Evaluation Team.
Photographs and Figure
 |
 |
 |
|
Figure 3. Baler Control Panel
|
The FACE investigation project is the cornerstone of the overall NIOSH program to prevent occupational fatalities. The objectives for this effort include the investigation of occupational fatalities to assess and characterize the circumstances of these events in order to develop succinct descriptive and evaluative reports for distribution to occupational safety and health groups across the country. This work is being conducted by the FACE investigation team. It is expected that the reports alone will have a major impact by better defining the causal factors behind occupational fatalities, calling national attention to the problem, and providing insights into the prevention efforts that are needed. However, the program does not determine fault or place blame on companies or individual workers.
- Page last reviewed: November 18, 2015
- Page last updated: October 15, 2014
- Content source:
- National Institute for Occupational Safety and Health Division of Safety Research