


Ethylene Oxide Sterilizers in Health Care Facilities: Engineering Controls and Work Practices
 ShareCompartir
ShareCompartir
July 1989
DHHS (NIOSH) Publication Number 89-115
Current Intelligence Bulletin 52
Foreword
Current Intelligence Bulletins (CIBs) are issued by the National Institute for Occupational Safety and Health (niosh), Centers for Disease Control (CDC), Atlanta, Georgia, to disseminate new scientific information about occupational hazards. A CIB may draw attention to a previously unrecognized hazard, report new data on a known hazard, or disseminate information on hazard control. Our intention is to make this information readily available to anyone who needs it. The documents are distributed to representatives of academia, industry, organized labor, public health agencies, and public interest groups as well as to Federal agencies responsible for ensuring the safety and health of workers.
CIBs are prepared by the staff of the Division of Standards Development and Technology Transfer, niosh (Robert A. Taft Laboratories, 4676 Columbia Parkway, Cincinnati, Ohio 45226). We welcome suggestions concerning the content, style, and distribution of these documents.
A Special Occupational Hazard Review published by niosh in 1977 concluded that occupational exposure to ethylene oxide (EtO) may increase the frequency of mutations in humans. This conclusion was based on (1) studies showing that changes occurred in the genetic material of cells following exposure to EtO, and (2) the observation that covalent chemical bonds were formed between EtO and deoxyribonucleic acid (DNA), which controls the genetic determination of all organisms. The information in the Special Occupational Hazard Review was updated in 1981 through a niosh CIB. The CIB was published after a study showed that EtO was carcinogenic in experimental animals and after reports demonstrated adverse reproductive effects in mammals.
Because the Occupational Safety and Health Administration (OSHA) has lowered the permissible exposure limit (PEL) for EtO and recently added an excursion limit, new strategies for hazard control axe essential. niosh has both conducted and reviewed recent research on engineering controls and work practices designed to protect workers employed near EtO sterilizers in health care facilities. The purpose of this bulletin is to disseminate recommendations for engineering controls and work practices to control exposure to EtO during the operation of gas sterilizers used in health care facilities.
niosh recommends that manufacturers of EtO sterilizers disseminate the information in this CIB to their customers, that employers make it available to their workers, and that professional and trade associations and unions inform their members of the engineering controls and work practices provided in this bulletin. Readers seeking more detailed information on the studies cited in this bulletin are urged to the original publications.
[signature]
J. Donald Millar, M.D., D.T.P.H. (Lond.)
Assistant Surgeon General
Director, National Institute for
Occupational Safety and Health
Centers for Disease Control
Abstract
This bulletin identifies potential sources of ethylene oxide (EtO) exposure from gas sterilizers in health care facilities and describes control methods recommended by the National Institute for Occupational Safety and Health (niosh). A complete system for controlling EtO exposures from gas sterilizers consists of both specific and general controls. The purpose of specific control methods such as the use of engineering controls, good work practices, and personal protective equipment is to protect workers at known and potential discharge points of EtO in the sterilizer system. General control methods such as equipment maintenance and workplace monitoring assure safe operation and provide timely feedback about the effectiveness of controls. Other general control methods include a good respiratory protection program and the labeling and posting of hazards.
Background
The National Institute for Occupational Safety and Health (niosh) recommended in 1981 that ethylene oxide (EtO) be regarded as a potential occupational carcinogen and that appropriate controls be used to reduce worker exposure [niosh 1981]. These recommendations were based primarily on an industry-sponsored study demonstrating that EtO was carcinogenic in experimental animals [Union Carbide Corporation 1981]. The niosh report also noted adverse reproductive effects in mammals and possible chromosomal aberrations in workers.
Since 1981, niosh has completed a cytogenetic study showing an increase in sister chromatid exchanges and chromosome aberrations in monkeys exposed to EtO [Lynch et al. 1984b]. niosh has also conducted a study showing statistically significant associations between EtO exposure and an increased incidence of rat neoplasms, including mononuclear cell leukemia, peritoneal mesothelioma, and mixed-cell glioma [Lynch et al. 1984a].
Evidence now available on reproductive toxicity suggests that EtO exhibits a dose-rate effect [Generoso et al. 1986]. Such an effect raises additional concerns about short-term exposures, even when they do not exceed the full-shift exposure limits.
Effective source control measures (i.e., containment or local ventilation) and work practices must therefore be implemented to reduce the potential for worker exposure. Because the odor of EtO cannot be detected until the concentration exceeds approximately 700 parts per million (ppm) [Clayton and Clayton 1978], significant exposures can occur without the worker's knowledge. This possibility emphasizes the need for an effective and reliable system of exposure control measures.
Purpose
niosh has studied techniques for controlling exposures from EtO sterilizers because a large number of health care workers are potentially exposed by this route. This publication discusses potential sources of EtO exposure and recommends protective measures that niosh researchers have observed to be effective in hospitals.
EtO Exposure Limits
In June 1984, the Occupational Safety and Health Administration (OSHA) promulgated a new standard for EtO that included a permissible exposure limit (PEL) of 1 ppm (1.8 mg/m3) measured as an 8-hour time-weighted. average (8-hr TWA) [Federal Register 1984]. The previous PEL was 50 ppm (90 mg/m3). In April 1988, OSHA amended its existing standard by adopting an excursion limit for EtO-- that is, no worker may be exposed to an airborne concentration that exceeds 5 ppm (9 mg/m3) as averaged over a sampling period of 15 min [Federal Register 1988].
niosh recommends (1) that a worker's exposure be limited to 5 ppm (9 mg/m3) EtO for no more than 10 min per workday, and (2) that the worker's 8-hr TWA exposure be limited to less than 0.1 ppm (0.18 mg/m3) EtO [niosh 1983]. This niosh recommended exposure limit (REL) is based on the conclusion that EtO is mutagenic and carcinogenic in animals and is also capable of causing adverse reproductive effects. niosh has also concluded that EtO causes chromosomal damage in humans and has the potential for causing cancer and adverse reproductive effects in humans [niosh 1983].
The American Conference of Governmental Industrial Hygienists (ACGIH) has designated EtO as an A2 substance (suspected human carcinogen). The ACGIH threshold limit value (TLV® ) for EtO is 1 ppm (2 mg/m3) as a TWA for a normal 8-hr workday and a 40-hr workweek [ACGIH 1988].
Extent of Occupational Exposure
Although less than 2% of EtO produced in the United States is used as a sterilant [Glaser 1977], most worker exposures result from this application [Federal Register 1983]. niosh estimated in 1977 that as many as 75,000 U.S. health care workers employed in sterilization operations may be directly exposed to EtO, and that an additional 25,000 workers may be incidentally exposed because of inadequate control measures [Glaser 1977].
Description of EtO Sterilizers
All gas sterilizers consist of an enclosed space where items are exposed to EtO for a sufficient period to sterilize them. The two types of gas sterilizers used in health care facilities are (1) automatic, general purpose sterilizers that are supplied by compressed-gas cylinders or single-dose cartridges, and (2) sterilizers that use glass ampules.
Automatic, General Purpose Sterilizers
Most hospital gas sterilizers may be classified as automatic, general purpose sterilizers [AAMI 1986]. They are constructed of metal and feature a gasketed door that locks when the sterilizer is in operation (see Figure 1). The majority of these units are pressurized during sterilization and use 12% EtO (by weight) and 88% dichlorodifluoromethane (refrigerant-12) supplied in compressed-gas cylinders. The EtO is mixed with dichlorodifluoromethane to reduce its flammability. Other automatic, general purpose sterilizers are not pressurized but operate below atmospheric pressure throughout the entire cycle and use small, single-dose cartridges of 100% EtO.
For the automatic, general purpose sterilizers, the basic sterilization cycle consists of the following phases:
- An initial chamber evacuation, humidification, and EtO charging phase
- A dwell period during which sterilization takes place
- A final chamber evacuation phase that may include aeration
Both pressurized and nonpressurized sterilizers may have vacuum purges at the end of the cycle. Most items are sterilized at 130°F (54.4°C) for about 2.5 hr, heat-sensitive items are sterilized at 100°F (37.8°C) for about 5 hr. Aeration typically takes 12 hr.
The pressurized sterilizers use a water-sealed vacuum pump to evacuate the chamber. To prevent siphoning from the drain, plumbing codes require an air gap where the discharge line from the pump empties into the floor drain. The single-dose cartridge sterilizers that use 100% EtO are fitted with a venturi vacuum pump driven by compressed air. The discharge line is usually vented outside the building through the roof or an exterior wall.
For all automatic, general purpose sterilizers, a buzzer indicates the completion of the basic cycle. At this point, the operator allows the sterilizers with in-chamber aeration to continue uninterrupted through the aeration mode. For loads that must be transferred to undergo aeration, the operator unloads the sterilizer and transfers the sterilized items to an aerator. This transfer may be done immediately at the end of the final evacuation cycle, or the operator may open the sterilizer door slightly and leave the area for approximately 15 min (the "door-cracked" period) before returning to transfer the load. Some sterilizers are fitted with a catch that permits the door to remain partially open for the "door-cracked" period. Once the door is fully opened, the load is removed from the sterilizer. In most cases, baskets used to transfer items are manually pulled from the shelves of the sterilizer chamber and carried to the aerator, where they ate set on shelves. Sterilized items may also be individually transferred to the aerator by hand, or they may be transported to the aerator in a cart.
Sterilizers that Use Glass Ampules
For EtO sterilizers that use glass ampules, the operator places wrapped or packaged items inside a plastic bag lining the container box. The operator then hand-breaks a single-use glass ampule of EtO and inert stabilizers inside the liner bag. (The ampule is encased in a plastic sheath and contained in a small, sealed plastic bag when it is broken.) The liner bag is then quickly collapsed to expel excess air and is sealed with a twist-tie. The container box is shut immediately to enclose the liner bag, which rapidly inflates as the EtO diffuses through the plastic sheath and the sealed plastic bag. During the sterilization period, EtO also diffuses through the liner bag and the container box into the room air. After 12 hr, the container and the liner bag are opened, and the items are removed for aeration.
Exposure Sources and Specific Control Methods
The following discussion deals with EtO exposure sources and control methods identified in niosh investigations of EtO exposures in hospitals [Kercher 1985a, 1985b; Kercher and Mortimer 1987; Mortimer and Kercher 1985a, 1985b, 1986; Mortimer et al. 1986; O'Brien 1985a, 1985b; Ringenburg et al. 1986; Todd et al. 1985]. Some EtO sources and controls are associated with all gas sterilizers, whereas others apply only to a particular type of sterilizer.
Sterilizer Area
Exposure Source
Sterilizer leaks can occur from the failure of gaskets, valves, or other equipment as well as from other sources described in this report. The layout of the sterilizer system can significantly affect the potential for EtO exposure if a leak should occur.
Control Methods
If a sterilizer is supplied by a gas cylinder (Figure 1), the sterilizer, cylinder, and associated piping should be contained in a mechanical access room (also called the equipment room or recess room). Access to the front of the sterilizer should be gained through a separate loading room. The loading room should not be routinely occupied when the sterilizer is operating. A window should allow direct observation of the loading area and control console. Sterilizers using cartridges or glass ampules should also be located in separate, ventilated rooms or in laboratory hoods that are appropriate for controlling EtO exposure.
Operation of Sterilizers
Supply Cylinders
Exposure Source.--Compressed-gas supply cylinders are potentially large sources of EtO exposure. A typical large supply cylinder of the 12:88 gas mixture contains 7,000 g of EtO. The supply line from such a cylinder contains liquid EtO under pressure. If this line is not properly purged before disconnection, the worker may be exposed to EtO from residual liquid or vapor in the supply fine [Mortimer and Kercher 1985a].
Control Methods.--To control the inhalation hazard, local exhaust ventilation should be provided above the supply cylinders where they are connected to the sterilizer supply line(s), or the supply cylinders should be enclosed in a ventilated cabinet.
To protect workers who must disconnect the supply cylinder, a three-way vent valve should be installed on the supply line where it connects to the cylinder shut-off valve. This three-way valve should direct residual EtO from the supply line to a dedicated exhaust ventilation system or to the ventilated enclosure around the evacuation line and drain air gap.
The EtO supply line from the tank to the sterilizer should also contain a pressure gauge. The supply valve, tank valve, and vent valve should be labeled; these labels should be consistent with the written operating instructions. When changing the supply cylinder or disconnecting any portion of the supply line, workers should wear a full-face shield, protective gloves, and other protective clothing as required by OSHA [29 CFR* 1910.1047] to protect any area of the body that may come in contact with liquid EtO. For maximum protection, the gloves should be made of nitrile or butyl rubber.
External EtO Cartridge Connection
Exposure Source.--Sterilizers with an external EtO cartridge connection place the worker at risk of being sprayed by or otherwise exposed to EtO when the cartridge is punctured [Ringenburg et al. 1986].
Control Method.--Use only those sterilizers that require the cartridge to be inside the chamber with the door closed before the cartridge can be punctured.
Newly Sterilized Loads
Exposure Sources.--Direct contact with EtO may occur when the operator transfers a load from the sterilizer to the aerator. A typical charge of EtO produces concentrations greater than 200,000 ppm in the sterilizer during the sterilization cycle. Grab samples taken during surveys showed concentrations up to approximately 4,000 ppm in the chamber when the door was first opened.
High EtO concentrations (10 to 100 ppm) can build up around newly sterilized, unaerated loads [Kercher and Mortimer 1987]. Workers may therefore increase their exposures significantly by close contact with such loads for more than a few seconds (unloading requires 1 to 2 min). For example, one niosh survey revealed that short-term exposures were 5 to 10 times greater than usual when operators transferred loads by holding the sterilized items on their arms close to their breathing zone [Kercher 1985b]. Other niosh hospital surveys [Ringenburg et al. 1986] revealed that unloading produced short-term EtO exposures of 5 to 100 ppm as a result of inadequate ventilation and unsafe work practices.
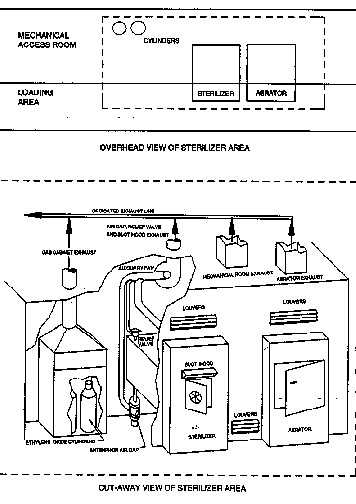
FIGURE 1. Gas-cylinder-supplied EtO sterilizer with isolated loading area and mechanical access room.
Control Methods.--For maximum protection, the concentration of EtO in the sterilizer chamber should be as low as possible before the worker opens the door and removes the load. To eliminate or greatly reduce exposure to newly sterilized loads, in-chamber aeration should be used if available. If it is necessary to transfer the load to achieve aeration, workers should run as many post-sterilization EtO-reduction cycles as time allows. To further reduce the chamber concentration of EtO before load transfer, a ventilated exhaust hood should be installed above the sterilizer door, and the door should be opened for 15 or 20 min to the latched position or to a distance of 2 inches, whichever is less.
Workers should spend minimal time in the loading area during the entire sterilization cycle and should be kept away from the area during the door-latched phase. Any handling of a newly sterilized load should be done carefully but as quickly as possible to minimize EtO exposure. The operator should maintain an arm's length distance from the load if possible. A cart should be used to transfer the load, and instead of pushing the load (which may force EtO into the breathing zone), the cart should be either pulled or pushed from the side.
Sterilizers that Use Glass Ampules
Exposure Sources.--Sterilizers that use glass ampules pose the risk of skin contact with liquid EtO when the operator breaks the ampule. EtO concentrations may be greater than 100,000 ppm inside the plastic liner bag during sterilization, depending on the quantity of EtO used and the volume of the liner bag. At the end of the 12-hr sterilization period, EtO concentrations in the bag may still range from 100 ppm to more than 1,000 ppm.
Control Methods.--Because of the potential for worker exposure, the use of this sterilization system is not recommended. However, if this system is used on an interim basis, all procedures involving EtO should be performed in a ventilated enclosure with a dedicated exhaust ventilation system. The enclosure should surround the equipment and should be small enough to prevent worker entry. The only opening should be at the front, where access is required. The opening should be no larger than is necessary for the operator's arms to fit inside the machine and perform all sterilization operations, starting with the breaking of the ampule inside the enclosure. The exhaust rate from the enclosure should be sufficient to maintain a 100-ft/min face velocity across the opening. To prevent skin contact with liquid EtO when the ampule is broken, operators should wear a full-face shield, impervious gloves made from protective nitrile or butyl rubber, and other protective clothing as required by OSHA [29 CFR 1910.1047].
After sterilization, the external container and liner bag should be open for 20 to 30 min before the items are transferred to the aerator. During this period, the container should be kept inside the ventilated enclosure and no one should be allowed near the front of the sterilizer. The liner bag should either be aerated with the sterilized items or kept inside the ventilated enclosure for a sufficient period to dissipate the EtO before it is discarded. The liner bag and the used ampule should be disposed of in an isolated trash receptacle outside the building--not in an indoor area.
Ventilation
Dedicated Exhaust System
Exposure Sources.--Ventilation is the principal means for controlling EtO emissions. If the primary EtO exhaust system involves ductwork that has inlets in other rooms of the building, EtO could be spread to these areas. Some sterilizers are fitted with an auxiliary fan to exhaust EtO from the primary emission points around the sterilizer and push the exhausted air into the ventilation system. For sterilizers that use an auxiliary fan, EtO may be forced out other inlet grilles in the ventilation system if the main fan does not have sufficient capacity for the additional exhaust flow from the sterilizer fan. Tbis problem was observed during a niosh health hazard evaluation in one hospital that had two sterilizers, each with an auxiliary fan [Zey et al. 1987]. When the auxiliary fans from both sterilizers were running during the sterilizer purge period, the capacity of the exhaust system was exceeded, and the EtO-laden air was forced out of the exhaust ventilation grilles and into an adjoining room.
Significant EtO exposures may occur if the ventilation sys- tem fails or if its performance deteriorates significantly. Without reliable ventilation system monitors and alarms, the sterilizer operator may be unaware of a malfunction. An accidental release of a large quantity of EtO could contaminate other areas of the facility through the general ventilation system.
Control Methods.--EtO exhaust should be vented to a dedicated exhaust ventilation system--that is, a system composed of local exhaust ducts that serve the sterilizer area only (i.e., the area containing the sterilizer, EtO cylinders, aerator, etc.) and route EtO directly to the outside of the building by maintaining a net suction on all of the exhaust ductwork. The exhaust system should be designed so that prevailing winds will not carry the exhaust into populated areas or into the open windows, doors, or air intakes of buildings [ASHRAE 1985]. If such a system has not yet been installed, and if the system uses one or more auxiliary fans, each grille in the system should be checked under all operating conditions with a smoke tube or other directional-flow indicator to ensure that air is drawn into the exhaust system and not pushed out while auxiliary fans are running.
Flow sensors and alarms should be installed to warn workers of fan failure or degraded performance. The sterilizer should not be operated if the exhaust system is not functioning property, and the sensor and alarm systems should be checked as recommended by the manufacturer to ensure that they are operating.
Local Exhaust for Sterilizer Door
Exposure Source.--Local exhaust ventilation above the sterilizer door will capture most of the EtO emitted from the partially open sterilizer door if the flow rate is adequate for the location of the exhaust hood [Kercher and Mortimer 1987]. However, when the sterilizer door is first opened, the hot air (100° to 130°F, or 37.8° to 54.4°C) rises and entrains room air. Some EtO may escape if the ventilation hood does not exhaust all of the air rising from the open sterilizer door.
Control Method.--The local exhaust ventilation hood should be located as close as possible to the top of the sterilizer door. The greater the distance above the door, the larger the hood will need to be and the more air it will need to draw. The hood should be designed to control the EtO under worst-case conditions, which occur when the door is first opened. Any test of the hood's capacity for containing EtO (e.g., workplace monitoring) should therefore be conducted when the sterilizer door is first opened.
To prevent contamination of other areas of the hospital, the ventilation system serving the EtO sterilizer room should have a dedicated exhaust system.
Ventilation Systems for Sterilizer Enclosures and Mechanical Access Rooms
Exposure Sources.--Sterilizers that are supplied by compressed-gas cylinders are often recessed into a wall of the sterilizer room. The sterilizer door is usually located in the sterilizer room, but the gas cylinders, drain enclosure, and other potential emission points of EtO are in an adjacent mechanical access room. Workers who must enter the mechanical access room should not be at excess risk of EtO exposure unless engineering controls we absent or operating improperly, or unless an accident occurs. If the ventilation malfunctions, workers are at greatest risk during the purge cycle of the sterilizer, when EtO-laden air is vented from the chamber. If the mechanical access room becomes contaminated, EtO may also escape into work areas through any vents or openings in the walls [Mortimer et al. 1986].
All sterilizers should be located in one mechanical access room with the loading area in an adjacent room. However, the niosh survey indicated that some sterilizers were not recessed but were free-standing and enclosed in a cabinet. EtO leaks inside these cabinets (which are not usually ventilated) can also lead to worker exposure [O'Brien 1985b].
Control Methods.--Exhaust ventilation should be such that the net flow of air is from the loading room to the mechanical access room, with a net flow of air into both rooms. In the mechanical access room, air should enter all openings in the upper portion of the enclosure with a face velocity of at least 50 to 100 ft/min. This velocity should be measured when all equipment in the enclosure is at operating temperature. Also, the ventilation should be sufficient to keep the temperature below 100ø F in the area where the EtO cylinders are located [niosh 1989]. To take advantage of the fact that heated air from the equipment will rise, the room exhaust should be located near the ceiling and the EtO supply should be located near the floor.
To alert workers that a purge cycle is in progress, a warning light should be placed at each entrance to the mechanical access room, and a flashing or revolving light should be placed inside the room. Workers should not enter the mechanical access room during the purge cycle without the appropriate respiratory protection. If a sterilizer is enclosed in a cabinet, the cabinet should be vented to a dedicated exhaust system.
Waste Discharges
Discharges From Buildings
Exposure Source.--When EtO is discharged from buildings, high concentrations can be carried for some distance on prevailing winds. Such EtO emissions can directly expose people downwind of the discharge, or they can enter the intakes of building heating, ventilation, and air conditioning systems [Buonicore 1984].
Control Method.--The exhaust ventilation discharge should be designed so that prevailing winds will not carry EtO, into populated areas, open windows, doors, or air intakes for the heating, ventilating, or air conditioning systems of any buildings. The ASHRAE Handbook [1985] contains detailed data on the design of ventilation systems. Any environmental release of EtO must comply with Federal, State, and local regulations.
Vacuum Pump and Sewer Drain Discharges
Exposure Sources.--During the evacuation phase for sterilizers that use compressed-gas cylinders, 90% to 99% of the EtO in the chamber is discharged into a drain through the water-sealed vacuum pump. Even if the drain air gap between the sterilizer evacuation line and the sewer drain pipe is enclosed and ventilated, significant quantities of EtO may be emitted if the ventilation flow fate is inadequate or if the plumbing from the vacuum pump to the trap in the sewer drain line is not sealed [Mortimer and Kercher 1985a, 1985b, 1986]. Another potential source of EtO is leakage from a small drain line connecting the leak-cups of the water-sealed vacuum pump to the floor drain [Mortimer and Kercher 1985b; Kercher 1985a].
Control Methods.--A ventilated enclosure should be placed around the air gap between the sterilizer evacuation line and the drain. Consult the sterilizer manufacturer for the proper exhaust ventilation rate. The vacuum pump discharge line should be installed to prevent water spillage. An air gap must be maintained between the discharge and the drain to avoid siphoning. The air gap should be partially enclosed, baffled, and ventilated. The floor drain junction should be sealed, as should all other connections of the sterilizer evacuation line and the drain line (except the openings into the ventilated enclosure).
Discharge Line from a Single-Dose Cartridge Sterilizer
Exposure Source.--Sterilizers that use single-dose cartridges may contain greater than 400,000 ppm EtO in the chamber during sterilization, depending on the quantity of EtO used and the volume of the chamber. During the evacuation phase, more than 55% of the EtO in the chamber win pass through the discharge line. Because this line is pressurized from the venturi vacuum pump to the discharge point, EtO could be forced out if there were any openings in the line.
Control Methods.--As prescribed in the written maintenance procedures, periodic checks should be made to ensure that there are no leaks in the discharge line.
Discharges from Sterilizer Pressure-Relief Valve
Exposure Source.--Pressurized sterilizers are fitted with pressure-relief valves. If this valve opens during the sterilization dwell period, EtO is emitted from its discharge point. Also, as air flows into the sterilizer from a vent line at the end of the vacuum purge, the line can become a leak point during the pressurization cycle if failure occurs.
Control Methods.--The pressure-relief valve and air vent line should be vented to the dedicated EtO ventilation system. Consult the sterilizer manufacturer for the proper tubing size and exhaust ventilation rate required to handle any discharge from this valve.
Accidental Releases
Exposure Sources
Accidental releases of EtO may occur from several sources, including glass ampules, cartridges, sterilizer discharge lines, and EtO supply cylinders. Glass ampules generally contain 4 to 18 g of EtO, and single-dose cartridges usually contain 67, 100, or 134 g of EtO, depending on their size. An 8.8-ft3 sterilizer uses a mixture of EtO (12% by weight) and dichlorodifluoromethane, and it discharges approximately 150 g of EtO into the drain during each purge cycle. A typical large supply cylinder for the 12:88 gas mixture contains 7,000 g of EtO.
Because the odor of EtO cannot generally be detected below approximately 700 ppm [Clayton and Clayton 1978], workers can be exposed to high concentration of this compound without knowing it. A relatively small quantity of EtO in an average room can create concentrations that are many times the exposure limit. For example, 1g of EtO can create a concentration of more than 20 ppm in a 10- by 10-ft room with an 8-ft ceiling.
Control Methods
To control accidental releases, the sterilizer, gas cylinders, and associated piping should be contained in a mechanical access room. All exhaust from this room should be routed to a dedicated exhaust ventilation system, which is described in the following section. Access to the front of the sterilizer for loading should be gained through a separate, dedicated loading area.
A thorough review of the design and operation procedures using a form of process hazard analysis is useful for anticipating equipment and work practice failures that could lead to accidental releases [AICHE 1985; World Bank 1988]. niosh has recently completed a hazard and operability study (a form of process hazard analysis) of an EtO sterilizer system that describes how this type of evaluation should be conducted [niosh 1989].
A written emergency response plan should be developed and practiced in anticipation of an accidental release. In the event of a known or suspected large release of EtO, the emergency response plan should be initiated. The area where the release occurred should be evacuated, and the appropriate personnel and departments should be notified (e.g., safety office, fire department, and maintenance crew). The area should be entered only by persons wearing pressure-demand, self-contained breathing apparatus until the problem is corrected and EtO concentrations return to acceptable levels. Sensors and alarms should be installed to detect and warn of accidental releases of EtO.
General Control Methods
Maintenance
Maintenance procedures and schedules vary among facilities, and therefore a written maintenance plan should be prepared for each facility that uses EtO sterilization equipment. The procedures should be developed by knowledgeable persons who consider the equipment manufacturers' recommendations, frequency of use, and other circumstances that might affect the integrity of the equipment. The maintenance plan should also include regular checks of door gaskets, valves, tubing, and piping connections. Maintenance workers should wear the proper personal protective equipment to prevent skin or inhalation exposures, as required in 29 CFR 1910.1047. They should also be aware of potential sources of EtO and procedures for avoiding exposure during maintenance.
Monitoring
Routine monitoring of the sterilizer and associated equipment as well as the work environment is needed to ensure the continuing effectiveness of engineering control measures, work practices, and equipment maintenance. Workplaces can be monitored for contaminants by using (1) conventional air sampling methods, which determine average concentrations over a period of time, or (2) real-time monitoring devices, which measure actual concentrations at a specific point or interval in time.
Conventional Air Sampling
Sampling Methods.--niosh recommends two air-sampling methods for EtO: Methods 1614 and 3702 [niosh 1987a, 1987b]. Method 1614 involves collecting EtO on a hydrogen-bromide-coated charcoal tube and measuring a derivative of EtO (2-bromoethylheptafluorobutyrate) by gas chromatography using an electron-capture detector. The detection limit of this method is 0.0006 ppm EtO per samples and the working range is 0.05 to 4.6 ppm. This method is applicable to short-term (10-min) samples.
niosh Method 3702 employs a direct-reading technique using a portable gas chromatograph with a photoionization detector. Samples are collected by drawing a known volume of air into a gas-sampling bag. Use of a sampling bag allows sampling times ranging from a few seconds to 8 hr. The working range of this method is 0.001 to 1,000 ppm in relatively noncomplex atmospheres such as those in the sterilizer areas of hospitals.
Sampling Strategies.--The most reasonable, efficient sampling strategy is to sample the worker with the highest risk of exposure [Leidel et al. 1977]. A maximum-risk worker should be selected and sampled for each operation that poses a risk of EtO exposure. Samples should be obtained during periods of maximum EtO concentration for comparison with ceiling standards. Periods of maximum EtO concentration should be determined by using all available knowledge about the area, workers, and process being sampled.
Real-Time Monitoring Devices
Real-time monitoring devices are an integral part of a control system for EtO. These devices include equipment-function sensors and environmental sensors.
Equipment-Function Sensors.--Equipment-function sensors are used to directly monitor the operation of the sterilizer and exhaust ventilation systems. Examples of these sensors are sail switches that indicate the presence of air flow in the ventilation exhaust ducts, and alarms or warning lights that indicate the sterilizer is in a purge cycle. Sensors should be connected to an audible alarm and a warning light to alert the operator to an equipment malfunction, or they may be designed to prevent sterilizer operation without the presence of exhaust ventilation [O'Brien 1985b].
Environmental Sensors.--Environmental sensors are gas sensors that monitor the atmosphere for the presence of EtO. These devices range from simple, low-cost, organic vapor sensors to complex gas chromatograph systems. Both the sterilizer room and the mechanical access room should be monitored and equipped with an alarm to warn workers of high EtO concentrations [Mortimer and Kercher 1985b, O'Brien 1985a].
Monitors do not need to be specific for EtO; for example, an organic vapor detector would be suitable. Gas chromatographic equipment may also be used to monitor EtO concentrations in the work environment. Frequent manual calibrations are required on systems without self-calibration. To avoid confusion, cylinders containing EtO should be stored apart from cylinders containing other gases. The sampling or detection points should be located approximately at breathing zone height, near the EtO cylinders, near the sterilizer body, and in the loading zone. Sampling lines should contain a rotameter or other flow indicator and should be inspected for damage routinely. Monitors should be tested at intervals recommended by the manufacturer.
Table I. NIOSH recommended respiratory protection for EtO
| Condition | Minimum respiratory protection*,** |
|---|---|
| Airborne concentration of <0.1 ppm | No respirator required |
| Airborne concentration of 0.1 to 5 ppm | Any air-purifying, full-facepiece canister respirator that provides protection against EtO and is equipped with an effective end-of-service-life indicator (ESLI), or
Any self-contained breathing apparatus (SCBA) equipped with a full facepiece, or Any supplied-air respirator (SAR) equipped with a full facepiece |
| Airborne concentration >5 ppm, or planned or emergency entry into unknown environments | Any SCBA equipped with a full facepiece and operated in a pressure-demand or other positive-pressure mode, or
Any SAR equipped with a full facepiece and operated in a pressure-demand or other positive-pressure mode in combination with an auxiliary SCBA operated in a pressure-demand or other positive-pressure mode |
| Firefighting | Any SCBA equipped with a full facepiece and operated in a pressure-demand or other positive-pressure mode |
| Escape only | Any air-purifying, full-facepiece canister respirator that provides protection against EtO and is equipped with an effective ESLI, or
Any appropriate escape-type SCBA |
*Only niosh/MSHA-approved equipment should be used. [return to table]
**The respiratory protection listed for any given condition is the minimum required to meet the niosh REL of 5 ppm (9 mg/m3) for no more than 10 min/day or <0.1 ppm (0.18 mg/m3) as an 8-hrTWA. [return to table]
Respiratory Protection
Respirators are the least preferred method for controlling worker exposure to EtO. They should not be used as the only means of preventing or minimizing exposure during routine operations, but they may be used in the following circumstances: when engineering and work practices are not technically feasible, when engineering controls are in the process of being installed, when emergencies occur, or when certain maintenance operations are being performed (including those requiring confined-space entry).
A respiratory protection program should include an evaluation of the worker's ability to perform the work while wearing a respirator, regular training of personnel, periodic environmental monitoring, and respirator fit testing, maintenance, inspection, and cleaning. Respirators should be selected by a knowledgeable person who is in charge of the program. The program must be evaluated regularly, and at a minimum, it must comply with the requirements of the OSHA respiratory protection standard [29 CFR 1910.134].
Workers should use only respirators that have been certified by niosh and the Mine Safety and Health Administration (MSHA). Table 1 lists the minimum respiratory equipment required to meet the niosh REL under given conditions. For additional information on the selection and use of respirators, consult the niosh Respirator Decision Logic [niosh 1987c] and the niosh Guide to Industrial Respiratory Protection [Bollinger and Schutz 1987].
Labeling and Posting of Hazards
Workers must be informed of exposure hazards, potential adverse health effects, and methods for protecting themselves from exposure to EtO. This information must be communicated in accordance with OSHA regulations as stipulated in 29 CFR 1910.1047 (Ethylene Oxide) and in 29 CFR 1910.1200 (Hazard Communication). In addition to the signs and labels required under, these regulations, niosh recommends that signs outlining good work practices be posted (1) in front of sterilizers, (2) above EtO supply cylinders, and (3) at the entrance to mechanical access rooms. Examples of these signs for automatic, general purpose sterilizers are printed at the end of this bulletin.
Note
*Code of Federal Regulations. See CFR in references. [return to text]
References
AAMI [1986]. Standard for automatic, general-purpose ethylene oxide sterilizers and ethylene oxide sterilant sources intended for use in health care facilities. Arlington, VA: Association for the Advancement of Medical Instrumentation.
ACGIH [1988]. TLV®s : threshold limit values and biological exposure indices for 1988-1989. Cincinnati, OH: American Conference of Governmental Industrial Hygienists.
AICHE [1985] Guidelines for hazard evaluation procedures. New York, NY: American Institute of Chemical Engineers.
ASHRAE [1985]. ASHRAE handbook: 1985 fundamentals. Atlanta, GA: Society of Heating, Refrigerating and Air-Conditioning Engineers, Inc., pp. 14.1-14.20.
Bollinger NJ, Schutz RH [1987]. niosh guide to industrial respiratory protection. U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control, National Institute for Occupational Safety and Health, DHHS (niosh) Publication No. 87-116.
Buonicore AJ [1984]. In-plant programs to reduce ethylene oxide worker exposure levels. Pharm Eng 4(4):35-41.
CFR. Code of federal regulations. Washington, DC: U.S. Government Printing Office, Office of the Federal Register.
Clayton GD, Clayton FE (eds.) [1978]. Patty's industrial hygiene and toxicology. 3rd ed. Vol. 2a, Toxicology. New York, NY: Wiley-Interscience, p. 2186.
Federal Register [1983]. 48 FR (No. 78): 17297, April 21, 1983. U.S. Department of Labor, 29 CFR, Pan 1910, Occupational exposure to ethylene oxide; proposed rule. Washington, DC: U.S. Government Printing Office, Office of the Federal Register.
Federal Register [1984]. 49 FR (No. 122): 25762, June 22, 1984. U.S. Department of Labor, 29 CFR, Part 1910, Occupational exposure to ethylene oxide; final standard. Washington, DC: U.S. Government Printing Office, Office of the Federal Register.
Federal Register [1988]. 53 PR (No. 185): 111414-111438, April 6,1988. U.S. Department of Labor, 29 CFR Part 1910, Occupational exposure to ethylene oxide; final standard. Washington, DC: U.S. Government Printing Office, Office of the Federal Register.
Generoso WD, Cain KT, Hughes LA, Sega GA, Braden PW, Gosslee DG, Shelby MD [1986]. Ethylene oxide dose and dose-rate effects in the mouse dominant-lethal test. Environ Mutagen 8:1-7.
Glaser ZR [1977]. Special occupational hazard review with control recommendations: use of ethylene oxide as a sterilant in medical facilities. Cincinnati, OH: U.S. Department of Health, Education, and Welfare, Public Health Service, Center for Disease Control, National Institute for Occupational Safety and Health, DHEW (niosh) Publication No. 77-200.
Kercher SL [1985a]. In-depth survey report: control technology for ethylene oxide sterilization in hospitals at Shriners Hospitals for Crippled Children, Burns Institute Cincinnati Unit, Cincinnati, Ohio, March 18-22,1985. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control, National Institute for Occupational Safety and Health, DHHS (niosh) Report 1985 (ECTB No. 146-18b), NTIS Publication No. PB-86-123866.
Kercher SL [1985b]. In-depth survey report: control technology for ethylene oxide sterilization in hospitals at Wooster Community Hospital, Wooster, Ohio. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control, National Institute for Service, Centers for Disease Control, National Institute for Occupational Safety and Health, DHHS (niosh) Report (ECTB No. 146-15b), NTIS Publication No. PB-87-163887.
Kercher SL, Mortimer V [1987]. Before and after: an evaluation of engineering controls for ethylene oxide sterilization in hospitals. Appl Ind Hyg 2(l):7-12.
Leidel NA, Busch KA, Lynch JR [1977]. Occupational exposure sampling strategy manual. Cincinnati, OH: U.S. Department of Health, Education, and Welfare, Public Health Service, Center for Disease Control, National Institute for Occupational Safety and Health, DHEW (niosh) Publication No. 77-173.
Lynch DW, Lewis TR, Moorman WJ, Burg JR, Groth DH, Khan A, Ackerman LJ, Cockrell BY [1984a]. Carcinogenic and toxicologic effects of inhaled ethylene oxide and propylene oxide in F344 rats. Toxicol Appl Pharmacol 76:69-84.
Lynch DW, Lewis TR, Moorman WJ, Burg JR, Gulati DK, Kaur P, Sabharwal PS [1984b]. Sister-chromatid exchanges and chromosome aberrations in lymphocytes from monkeys exposed to ethylene oxide and propylene oxide by inhalation. Toxicol Appl Pharmacol 76:85-95.
Mortimer V, Kercher SL [1985a]. In-depth survey report: control technology for ethylene oxide sterilization in hospitals at Bethesda Hospital, Cincinnati, Ohio. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control, National Institute for Occupational Safety and Health, DHHS (niosh) Report (ECTB No. 146-11b), NTIS Publication No. PB-87-164513.
Mortimer V, Kercher SL [1985b]. In-depth survey report: control technology for ethylene oxide sterilization in hospitals at Bronson Methodist Hospital, Kalamazoo, Michigan. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control, National Institute for Occupational Safety and Health, DHHS (niosh) Report (ECTB No. 146-13b).
Mortimer VD, Kercher SL [1986]. In-depth survey report: modified control technology for ethylene oxide sterilization in hospitals at Community Med Center Hospital, Marion, Ohio. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control, National Institute for Occupational Safety and Health, DHHS (niosh) Report (ECTB No. 146-12c), NTIS Publication No. PB-86-237252.
Mortimer VD, Kercher SL, O'Brien DM [1986]. Effective controls for ethylene oxide: a case study. Appl Ind Hyg 1(1):15-20.
niosh [1981]. Current Intelligence 35: Ethyene oxide (EtO). Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control, National Institute for Occupational Safety and Health, DHHS (niosh) Publication No. 81-130.
niosh [1983]. niosh Testimony to the U.S. Department of Labor, Occupational Safety and Health Administration proposed rule: occupational exposure to ethylene oxide. niosh policy statements. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control, National Institute for Occupational Safety and Health.
niosh [1987a]. niosh manual of analytical methods. Ethylene oxide. Method 1614. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control, National Institute for Occupational Safety and Health.
niosh [1987b]. niosh manual of analytical methods. Ethylene oxide. Method 3702. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control, National Institute for Occupational Safety and Health.
niosh [1987c]. niosh respirator decision logic. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control, National Institute for Occupational Safety and Health, DHHS (niosh) Publication No. 87-108.
niosh [1989]. Technical report control technology for ethylene oxide sterilization in hospitals. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control, National Institute for Occupational Safety and Health, DHHS (niosh) Publication No. 89-118.
O'Brien DM [1985a]. In-depth survey report: control technology for ethylene oxide sterilization in hospitals at Euclid General Hospital, Euclid, Ohio. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control, National Institute for Occupational Safety and Health, DHHS (niosh) Report (ECTB No. 146-14b), NTIS Publication No. PB-87-164497.
O'Brien DM [1985b]. In-depth survey report: control technology for ethylene oxide sterilization in hospitals at St. Francis/St. George Hospital, Cincinnati, Ohio. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control, National Institute for Occupational Safety and Health, DHHS (niosh) Report (ECTB No. 146-17b), NTIS Publication No. PB-86-125200.
Ringenburg VL, Elliott LJ, Morelli-Schroth P, Molina D [1986]. Industrial hygiene characterization of ethylene oxide exposures of hospital and nursing home workers. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control, National Institute for Occupational Safety and Health, DHHS (niosh) Report.
Todd WF, Kercher SL, Mortimer VD, O'Brien DM [1985]. In-depth survey report: control technology for ethylene oxide sterilization in hospitals at Community Med Center Hospital, Marion, Ohio. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control, National Institute for Occupational Safety and Health, DHHS (niosh) Report (ECTB No. 146-12b), NTIS Publication No. PB-86-116969.
Union Carbide Corporation [1981]. Section 8e [Toxic Substances Control Act] report: final report on ethylene oxide two-year inhalation study on rats. Project Report 44-20, Bushy Run Research Center (formerly Carnegie-Mellon Institute of Research), January 28,1981. Washington, DC: U.S. Environmental Protection Agency, Office of Toxic Substances. Unpublished report.
World Bank [1988]. Techniques for assessing industrial hazards: a manual. Washington, DC: The World Bank, World Bank Technical Paper Number 55.
Zey JN, Mortimer V, Elliott L [1987]. Evaluation of ethylene oxide exposures in a hospital sterilization unit. Paper presented at the 1987 All-Ohio Safety and Health Congress and Exhibit, Cleveland, Ohio, April 9,1987. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control, National Institute for Occupational Safety and Health, DHHS (niosh) Report (ECTB No. 146-12c), ISMS Publication No. PB-86-237252.
Work Practice Guidelines For Ethylene Oxide Sterilizers: Post by Sterilizer
DANGER! ETHYLENE OXIDE CANCER AND REPRODUCTIVE HAZARD
- Be sure that the sterilizer ventilation system is operating before the sterilizer is started and while the sterilizer is operating.
- Use in-chamber aeration when possible.
- If a sterilizer load must be transferred to an aerator, take the following precautions:
- After the sterilizer completes the required number of purge/aeration cycles, keep the load in the sterilizer for as many additional purge/aeration cycles as time allows.
- Make sure the local exhaust ventilation above the sterilizer door is working.
- Open the sterilizer door to the notched position (or 2 inches if there is no notched position) and leave the area for 15 minutes.
- Perform the load transfer as quickly as possible and keep the load as far away from your face as possible.
- In case of an ethylene oxide leak or other emergency, evacuate the area and initiate the emergency response plan. DO NOT RE-ENTER THE AREA WITHOUT A SUPPLIED-AIR RESPIRATOR!
Work Practice Guidelines For Ethylene Oxide Sterilizers: Post Above Ethylene Oxide Supply Cylinders
- Before changing cylinders, make sure the local exhaust ventilation for the cylinder is working.
- When changing cylinders, wear a full faceshield, protective gloves, and other protective clothing as required by OSHA (29 CFR 1910.1047).
- Before disconnecting the supply line from the cylinder valve, relieve excess pressure by venting the supply line into the ventilation system.
- In case of an ethylene oxide leak or other emergency, evacuate the area and initiate the emergency response plan. DO NOT RE-ENTER THE AREA WITHOUT A SUPPLIED-AIR RESPIRATOR!
Work Practice Guidelines for Ethylene Oxide Sterilizers: Post at the Entrances of Mechanical Access Rooms
- CAUTION! This room may contain a high concentration of ethylene oxide.
- In case of an ethylene oxide leak or other emergency, evacuate the area and initiate the emergency response plan. DO NOT RE-ENTER THE AREA WITHOUT A SUPPLIED-AIR RESPIRATOR!
- Page last reviewed: June 6, 2014
- Page last updated: June 6, 2014
- Content source:
- National Institute for Occupational Safety and Health Education and Information Division