

Recommended Definition of Initial Injury Visits to Emergency Departments for Use With the NHAMCS-ED Data
 ShareCompartir
ShareCompartir
by Lois A. Fingerhut, M.A., Office of Analysis and Epidemiology
A uniform method for identifying injury visits to emergency departments (EDs) for the states that collect ED data does not exist. Further, the definition currently used by the National Hospital Ambulatory Medical Care Survey — Emergency Department (NHAMCS-ED) component is too broad for states to replicate, and hence to use as a benchmark. This brief report provides a definition that focuses on initial injury visits that can be used as a benchmark for states that have state level ED data on injury diagnoses, external causes, and initial visit status. National estimates of injury-related ED visits based on different definitions of injury are compared.
Data sources
Four estimates of the number of injury visits based on the National Center for Health Statistics (NCHS) NHAMCS-ED component (1) and one estimate from the National Electronic Injury Surveillance System-All Injury Program (NEISS-AIP)—whose data are provided in the Web-based Injury Statistics Query and Reporting System, known as WISQARS (2)—were prepared for comparison. Both NHAMCS-ED and NEISS-AIP are designed to produce national estimates of injury visits seen in EDs. However, the two differ in survey methods. NHAMCS-ED data can be used to provide national estimates of injury-related visits that are based on a broad definition, whereas the NEISS-AIP was designed to provide national estimates of the initial visit for an injury episode. NEISS-AIP does not estimate injured people per se; a person could experience two or more separate injury episodes and be treated at the same NEISS hospital in the same year and be counted twice, although this rarely occurs. [Personal communication, Lee Annest, NCIPC, CDC, August 21, 2006]
Recommended definition of ED initial injury visit
Include initial visits to an ED for an injury episode with either: (a) a first-listed injury diagnosis based on the Barell matrix definition of an injury (3), regardless of any mention of an external cause-of-injury code; or (b) the first-listed valid external cause-of-injury code, based on the recommended framework for external causes of injury. For more information see, valid external cause codes and categories. Complications of care and adverse effects are excluded from both the diagnosis codes as well as the external cause codes because both the Barell matrix and the external cause of injury matrix, which are used internationally to categorize injury diagnoses and mechanisms of injury, exclude them. It has been generally accepted that these conditions are not amenable to the traditional work of state injury prevention programs (4).
The current NHAMCS-ED definition of injury-related visits, referred to as the traditional approach in this report, includes complications of care and adverse effects. In 2004, of all NHAMCS-ED defined injury-related visits, 3% of first-listed diagnosis codes and 4% of first-listed external cause-of-injury codes were for complications of care or adverse effects.
ED visits are often used as an estimate of the burden of injury. The definition historically used by NCHS includes a broad range of injury-related visits and can be viewed as a measure of burden on the health care system. By contrast, the recommended definition described here is incidence-based; it identifies only initial visits for a narrower range of external causes and diagnoses. Under the traditional approach, 38% of all visits to EDs in the U.S. were classified as injury-related in 2004, a proportion that has been constant since 1995. Using the recommended definition, 28% of all visits reflect initial visits for injuries.
Rationale for an incidence-based ED injury visit definition
The rationale for modifying the NHAMCS standard definition is based, in part, on the need to increase the relevance of the national statistics by using a methodology that can be replicated at the state level. To this end, ED data systems and availability of specific types of data have been considered. Specifically, the following points were considered:
- All states that have ED visit data available, have the ability to define a first-listed injury diagnosis (e.g., a fracture or an internal organ injury) based on the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) injury diagnosis codes.
- A consensus definition of injury for use in statewide hospital discharge datasets was published in 2003 (5). The codes used to define diagnoses are the same in both EDs and inpatient settings. For more information see, valid injury diagnosis codes and categories.
- Some states can identify external causes of injury (e.g., motor vehicle crashes, falls, and firearm-related injuries) using ICD-9-CM, and hence should include visits with the relevant external cause codes (5). States that cannot identify external causes of injury visits are encouraged to add that information to their dataset. for more information see, valid external cause codes and categories.
- Although most states are not currently able to identify whether an ED visit was an initial or follow-up visit, we believe that estimating incidence is preferable when possible. This brings estimates based on the recommended definition closer to the estimated number of people who visit EDs for different injuries than does the traditional approach. Because states that do not have the ability to identify initial visits will overestimate incidence of injuries, the recommendation still has merit for encouraging states to add a variable to their dataset that will allow them to identify initial visits.
Comparisons of ED injury visit estimates using different definitions
Table 1 [PDF – 19 KB] presents national estimates based on each definition, related ratios, and percentages of all ED visits for 1995-2004. Table 2 [PDF – 19 KB] provides an example of how an estimate based on the recommended definition was derived from the NHAMCS-ED data using variables for episode, first-listed diagnosis, and first-listed external cause code.
The recommended definition for initial injury visits is similar to the number of initial visits in EDs for injuries as estimated in the NEISS-AIP data (Table 1 [PDF – 19 KB] ). In 2004, these two numbers differed by only 5% compared with a 32% difference between the published NHAMCS-ED number of injury visits and the number of incidence-based injury visits.
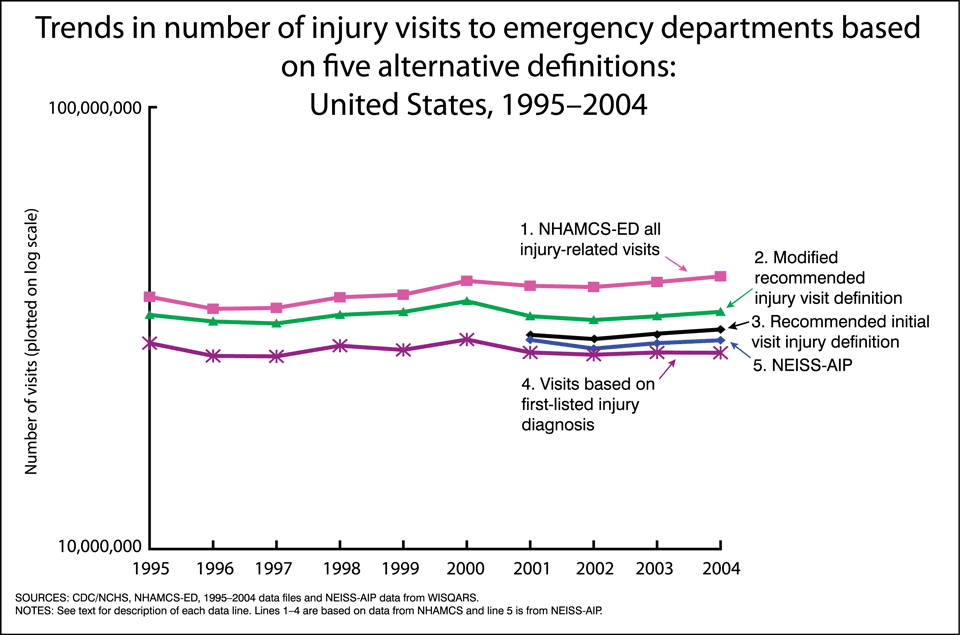
The Figure shows the trends in ED visits based on the various definitions of injury. The first four definitions refer to trends using the NHAMCS-ED data. The data lines are defined as follows:
Data line 1 – This is the standard definition used by the Ambulatory Care Statistics Branch that is responsible for the NHAMCS-ED survey. The definition of an injury visit is very broad, in an attempt to measure the full burden of injury including adverse effects and complications of care. The definition includes any mention of a reason for visit related to an injury, any of three diagnosis fields with an ICD-9-CM code in the range of 800-999 or any mention of an external cause of injury coded to E800-E999, or if the checkbox was “yes” for “Is visit related to injury, or poisoning, or adverse effect of medical treatment?”
Data line 2 – This modified version of the recommended injury visit definition does not include “initial visit” status because that variable did not become part of the NHAMCS-ED dataset until 2001. See “3” below. This trend line is useful for those states that cannot identify initial visits in their datasets, but who want a benchmark to national data using injury diagnoses and external cause-of-injury codes.
Data line 3 – Injury visits are defined as an initial visit to an ED with either a first-listed injury diagnosis regardless of any mention of an external cause-of-injury code or an initial visit with a valid external cause-of-injury code. Visits with a first-listed diagnosis code or external cause-of-injury code of either complications of care or an adverse effect are excluded. This is the recommended definition for use whenever a state wants a national benchmark and for having a closer estimate of the number of people who seek care in EDs for injuries.
Data line 4 – Injury visits are defined as having a first-listed injury diagnosis using the same definition as recommended for hospital discharge data. This definition excludes visits if the first-listed diagnosis is either a complication of care or an adverse effect. All states that collect ED data should be able to collect this information (3).
Data line 5 – The data are from the NEISS-AIP as reported by the National Center for Injury Prevention and Control and can be found on the WISQARS website. (2). They are shown for comparison to the NHAMCS-ED data.
References
- McCaig L, E Nagwar. National Hospital Ambulatory Medical Care Survey: 2004 emergency department summary. Advance data from vital and health statistics; no 372. National Center for Health Statistics. Hyattsville, MD. 2006.
- Centers for Disease Control and Prevention. Web-based Injury Statistics Query and Reporting System (WISQARS) [Online]. (2003) National Center for Injury Prevention and Control (producer). August 2006.
- Barell V, Aharonson-Daniel L, et al. An introduction to the Barell body region by nature of injury diagnosis matrix. Inj Prev 8(2): 91-6. 2002.
- Centers for Disease Control and Prevention. Recommended framework for presenting injury mortality data. 46(No. RR-14). 1997.
- Injury Surveillance Workgroup. Consensus recommendations for using hospital discharge data for injury surveillance. Marietta, Ga., State and Territorial Injury Prevention Directors Association. 2003.
Figures
- Page last reviewed: November 6, 2015
- Page last updated: April 6, 2010
- Content source: