

Racial and Ethnic Disparities in Men’s Use of Mental Health Treatments
 ShareCompartir
ShareCompartir
NCHS Data Brief No. 206, June 2015
On This Page
- Key findings
- Nearly 9% of U.S. men reported daily feelings of anxiety or depression, but the rate differed by race and ethnicity.
- Racial and ethnic differences in daily feelings of anxiety or depression were observed only for men aged 18–44.
- About 4 in 10 men with daily feelings of anxiety or depression took medication for these feelings or talked to a mental health professional, but the rate differed by race and ethnicity.
- Racial and ethnic differences in the use of mental health treatments by men with daily feelings of anxiety or depression were observed only for men aged 18–44.
- Among men aged 18–44, racial and ethnic differences in the use of mental health treatments were significantly greater for men without health insurance coverage than for men with health insurance.
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
PDF Version (724 KB)
Stephen J. Blumberg, Ph.D.; Tainya C. Clarke, Ph.D.; and Debra L. Blackwell, Ph.D.Key findings
Data from the National Health Interview Survey, 2010–2013
- Nearly 9% of men (8.5%) had daily feelings of anxiety or depression. Less than one-half of them (41.0%) took medication for these feelings or had recently talked to a mental health professional.
- Racial and ethnic differences were observed only for men aged 18–44.
- Among men aged 18–44, non-Hispanic black and Hispanic men (6.1%) were less likely than non-Hispanic white men (8.5%) to report daily feelings of anxiety or depression.
- Among men aged 18–44 who had daily feelings of anxiety or depression, non-Hispanic black and Hispanic men (26.4%) were less likely than non-Hispanic white men (45.4%) to have used mental health treatments.
- The significant racial and ethnic disparity in treatment utilization was associated with lack of health insurance coverage.
Compared with white Americans, persons of other races in the United States are less likely to have access to and receive needed mental health care (1–4). Few studies, however, have explored such disparities specifically among men. Mental health and treatment have traditionally received less attention for men than women, perhaps because men are less likely than women to report mental health problems and to receive services for these problems (4–7). This report uses nationally representative data on frequency of mental health symptoms and related treatment utilization to compare men of color (that is, non-Hispanic black and Hispanic men) with non-Hispanic white men. It also explores whether racial and ethnic disparities differ by age, health insurance coverage status, and income.
Keywords: men’s health, behavioral health, anxiety, depression
Nearly 9% of U.S. men reported daily feelings of anxiety or depression, but the rate differed by race and ethnicity.
Figure 1. Men aged 18 and over with daily feelings of anxiety or depression, by race and ethnicity: United States, 2010–2013
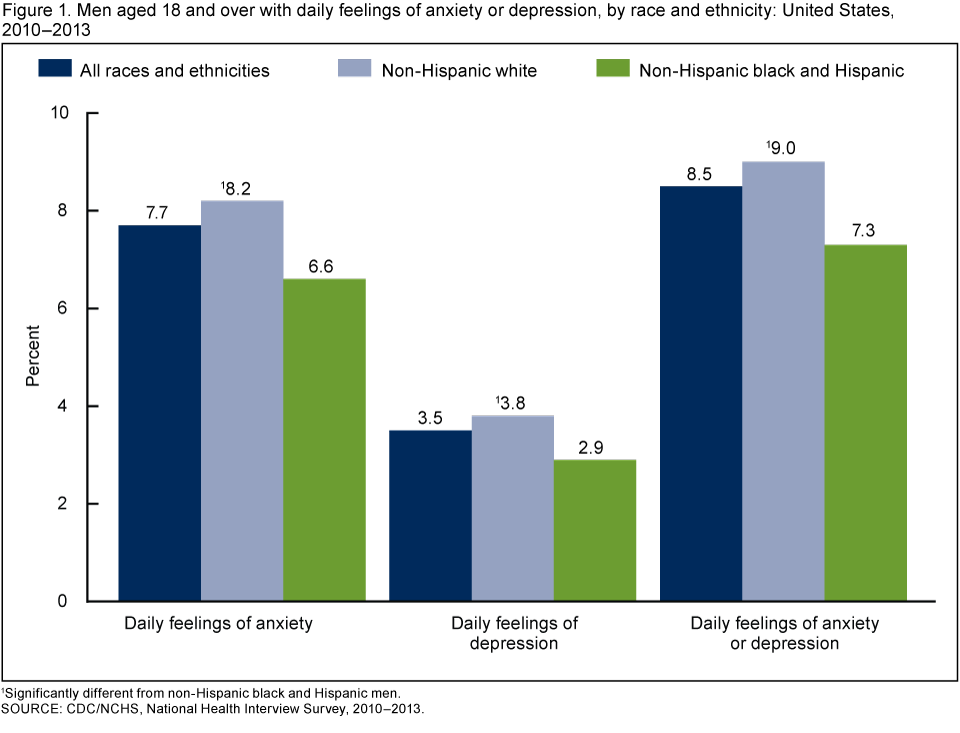
1Significantly different from non-Hispanic black and Hispanic men.
SOURCE: CDC/NCHS, National Health Interview Survey, 2010–2013.
Among all men aged 18 and over, 7.7% had daily feelings of anxiety, 3.5% had daily feelings of depression, and 8.5% felt either anxious or depressed every day (Figure 1). However, non-Hispanic black and Hispanic men (7.3%) were significantly less likely than non-Hispanic white men (9.0%) to feel anxious or depressed every day.
Racial and ethnic differences in daily feelings of anxiety or depression were observed only for men aged 18–44.
Men aged 18–44 (7.6%) were significantly less likely than men aged 45 and over (9.4%) to have daily feelings of anxiety or depression (Figure 2). This difference was due largely to racial and ethnic differences in the younger age group. Among those aged 18–44, non-Hispanic black and Hispanic men (6.1%) were nearly 30% less likely than non-Hispanic white men (8.5%) to have daily feelings of anxiety or depression. Among men aged 45 and over, there were no racial or ethnic differences in the prevalence of men with daily feelings of anxiety or depression.
Figure 2. Men aged 18 and over with daily feelings of anxiety or depression, by age and race and ethnicity: United States, 2010–2013
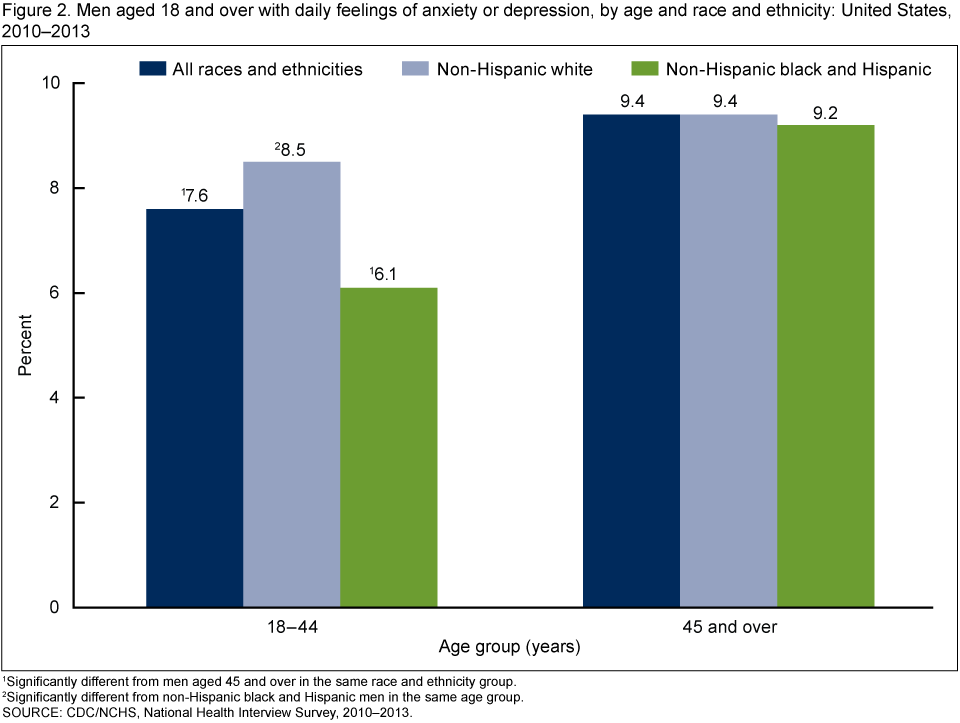
1Significantly different from men aged 45 and over in the same race and ethnicity group.
2Significantly different from non-Hispanic black and Hispanic men in the same age group.
SOURCE: CDC/NCHS, National Health Interview Survey, 2010–2013.
About 4 in 10 men with daily feelings of anxiety or depression took medication for these feelings or talked to a mental health professional, but the rate differed by race and ethnicity.
One in three men (33.0%) with daily feelings of anxiety or depression took medication for those feelings, and just over one-quarter (25.7%) talked to a mental health professional within the previous 12 months (Figure 3). Among men with daily feelings of anxiety or depression, non-Hispanic white men (43.0%) were more likely than non-Hispanic black and Hispanic men (36.0%) to have used either of these mental health treatments.
Figure 3. Men who used selected types of mental health treatments, among men aged 18 and over who felt anxious or depressed every day, by race and ethnicity: United States, 2010–2013
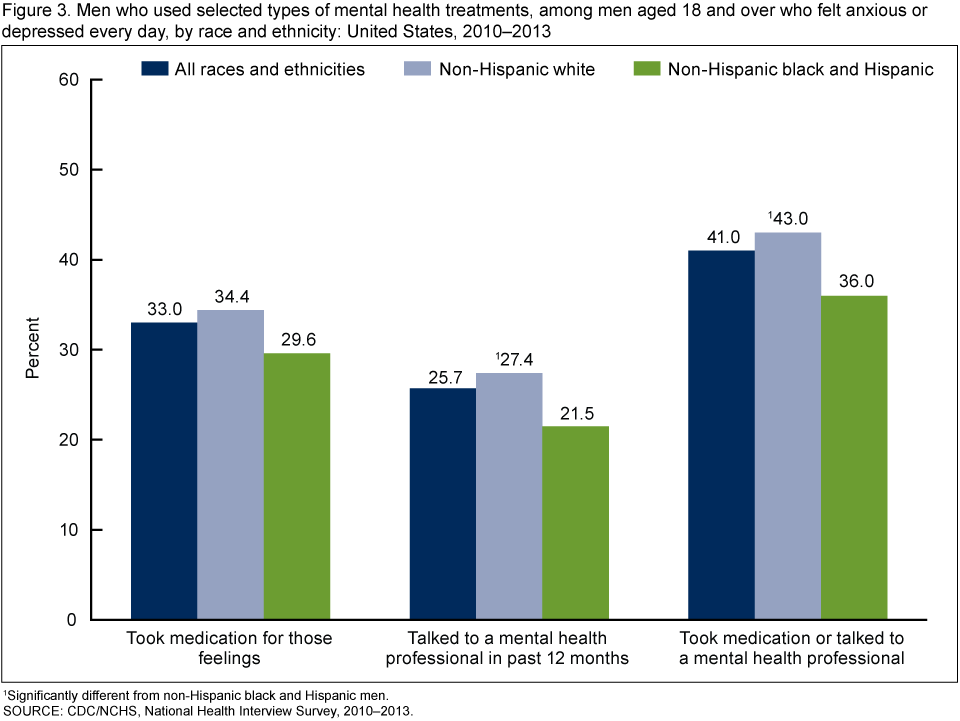
1Significantly different from non-Hispanic black and Hispanic men.
SOURCE: CDC/NCHS, National Health Interview Survey, 2010–2013.
Racial and ethnic differences in the use of mental health treatments by men with daily feelings of anxiety or depression were observed only for men aged 18–44.
Among men who felt anxious or depressed on a daily basis, younger men aged 18–44 (39.2%) were as likely as older men aged 45 and over (42.3%) to have taken medication for these feelings or to have seen a mental health professional in the previous 12 months (Figure 4). However, racial and ethnic differences in the use of mental health treatments were observed among men aged 18–44 with daily feelings of anxiety or depression. In this age group, non-Hispanic black and Hispanic men (26.4%) were about 40% less likely than non-Hispanic white men (45.4%) to have used mental health treatments. Race and ethnicity were not associated with use of mental health treatments among men aged 45 and over with daily feelings of anxiety and depression.
Figure 4. Men who took medication or talked to a mental health professional, among men aged 18 and over who felt anxious or depressed every day, by age and race and ethnicity: United States, 2010–2013
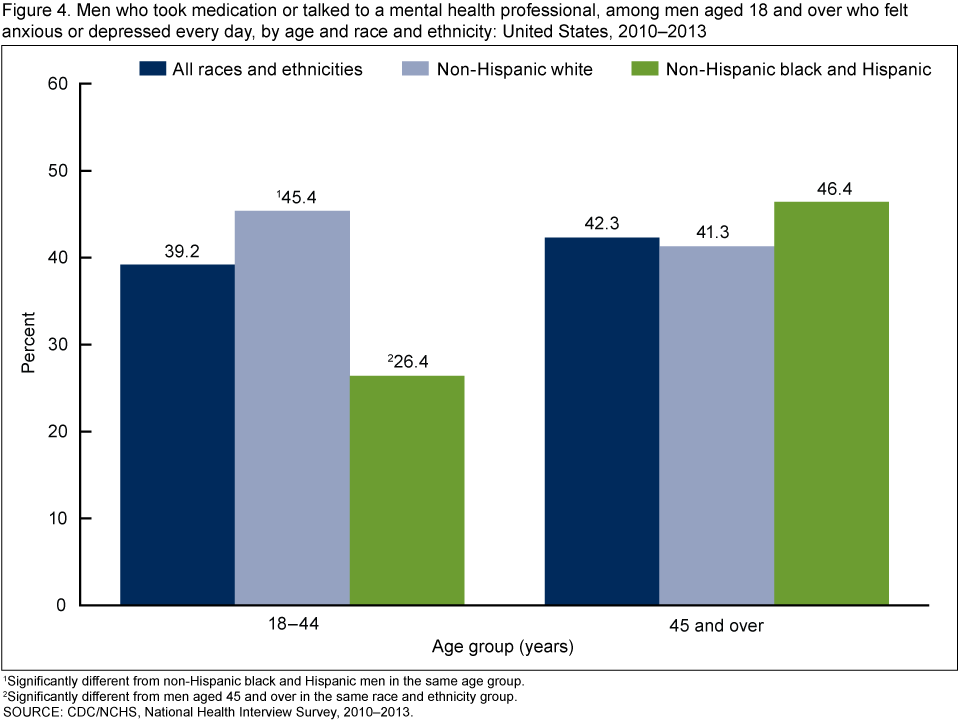
1Significantly different from non-Hispanic black and Hispanic men in the same age group.
2Significantly different from men aged 45 and over in the same race and ethnicity group.
SOURCE: CDC/NCHS, National Health Interview Survey, 2010–2013.
Among men aged 18–44, racial and ethnic differences in the use of mental health treatments were significantly greater for men without health insurance coverage than for men with health insurance.
Among uninsured men aged 18–44 with daily feelings of anxiety or depression, non-Hispanic white men (39.3%) were three times as likely as non-Hispanic black and Hispanic men (12.7%) to have used mental health treatments (Figure 5). This disparity was significantly smaller for men aged 18–44 who had health insurance coverage. In fact, among insured men aged 18–44 with daily feelings of anxiety or depression, no statistical difference was observed between the racial and ethnic groups in the use of mental health treatments.
In contrast, racial and ethnic disparities in use of mental health treatments were observed regardless of family income. Among men aged 18–44 who felt anxious and depressed every day, non-Hispanic white men were 1.7 to 2.0 times as likely as non-Hispanic black and Hispanic men to have taken medication or talked to a mental health professional.
Figure 5. Men who took medication or talked to a mental health professional, among men aged 18–44 who felt anxious or depressed every day, by health insurance coverage status, income, and race and ethnicity: United States, 2010–2013
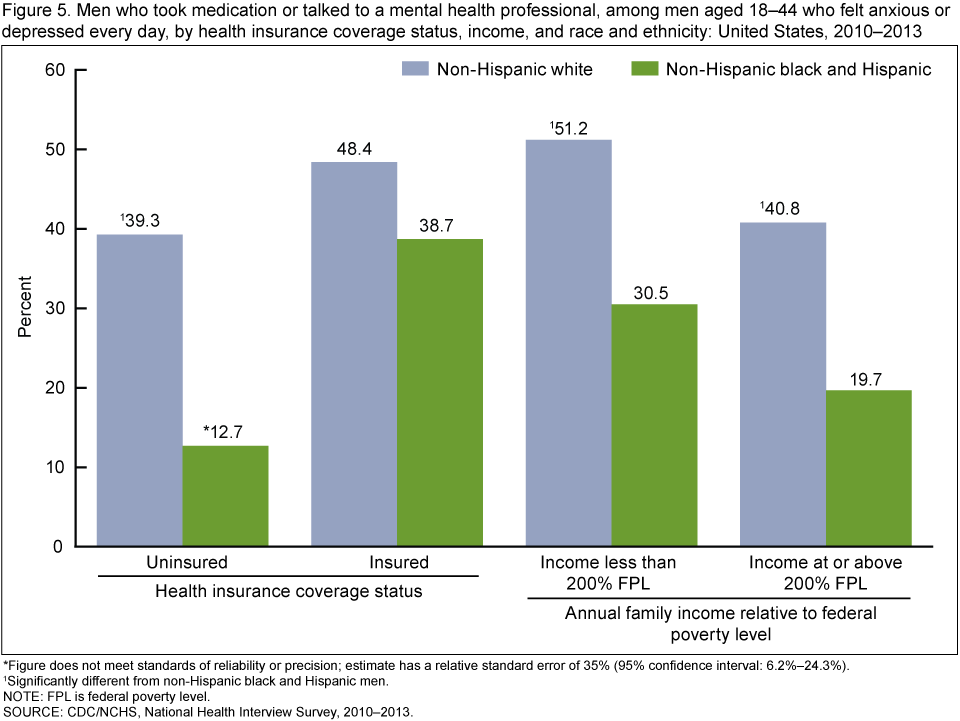
* Figure does not meet standards of reliability or precision; estimate has a relative standard error of 35% (95% confidence interval: 6.2%–24.3%).
1Significantly different from non-Hispanic black and Hispanic men.
NOTE: FPL is federal poverty level.
SOURCE: CDC/NCHS, National Health Interview Survey, 2010–2013.
Summary
Non-Hispanic black and Hispanic men were less likely than non-Hispanic white men to report having daily feelings of anxiety or depression, and this disparity was due to significant differences among younger men aged 18–44. This finding may seem to contradict other research revealing that rates of serious psychological distress (6) and depressive symptoms (7) are higher among Hispanic and non-Hispanic black persons than among non-Hispanic white persons. However, the findings in this report are based on a different measure of mental health symptoms (reported daily feelings) that considers frequency but not intensity of feelings. The findings in this report are also based on a different population (men only).
Younger men of color who reported daily feelings of anxiety or depression were less likely than their non-Hispanic white peers to take medication or talk to a mental health professional. This difference in treatment use was not observed for older men. Among the younger men, the racial and ethnic difference in treatment use was observed regardless of income.
Racial and ethnic differences in men’s mental health treatment use appear to be driven by differences among younger uninsured men. The survey data cannot be used to determine if young men of color without health insurance, relative to young uninsured non-Hispanic white men, perceive less need for treatment, are less motivated to seek treatment, experience additional non-cost barriers when attempting to access mental health treatments, or more quickly stop using treatments that do not seem to be working. In focus groups, young men of color were particularly likely to say that mental illness and treatment seeking are signs of weakness and can bring shame and embarrassment to one’s self and family (8). Yet having health insurance coverage appeared to reduce the impact of such barriers; the observed racial and ethnic difference in treatment use was significantly smaller for younger insured men. Recent expansions of health insurance coverage may consequently reduce these racial and ethnic disparities.
Definitions
Daily feelings of anxiety or depression: Based on responses to the survey questions, “How often do you feel worried, nervous, or anxious?” and “How often do you feel depressed?” Answer choices were daily, weekly, monthly, a few times a year, or never.
Mental health treatments: Based on responses to the survey questions, “Do you take medication for these feelings?” and “During the past 12 months, have you seen or talked to any of the following health care providers about your own health ... A mental health professional such as a psychiatrist, psychologist, psychiatric nurse, or clinical social worker?”
Family income relative to federal poverty level: Based on family income, family size, and age using the U.S. Census Bureau’s poverty thresholds for the previous calendar year. Imputed income files were used when income was missing.
Health insurance coverage status: Insured men include those who, at the time of interview, had any private health insurance, Medicare, Medicaid, Children’s Health Insurance Program, a state-sponsored or other government-sponsored health plan, or a military plan. Men were defined as uninsured if they did not have any of these coverage types, had only Indian Health Service coverage, or had only a private plan that paid for one type of service, such as accidents or dental care.
Race and ethnicity: Ethnicity refers to Hispanic or Latino origin, and persons of Hispanic or Latino origin may be of any race. For conciseness, this report used shorter versions of the 1997 Office of Management and Budget terms for Hispanic or Latino origin and race. For example, the category “not Hispanic or Latino, white, single race” is referred to as “non-Hispanic white.”
Data source and methods
The National Health Interview Survey (NHIS) is a multipurpose cross-sectional health survey that is fielded continuously by the Centers for Disease Control and Prevention’s (CDC) National Center for Health Statistics. Interviews are conducted in respondent’s homes, with telephone follow-up permitted if necessary. Analyses in this report were based on mental health and medication use data collected from a combined sample of 21,058 men aged 18 and over as part of the 2010 Quality of Life (QOL) and the 2011, 2012, and 2013 Adult Functioning and Disability (AFD) supplements to NHIS. Demographic and other health information (including contact with mental health professionals) were collected in the Household, Sample Adult Core, and Family Core components of NHIS. The QOL and AFD supplements were administered for a random subsample of NHIS sample adult respondents. For more information about NHIS visit its website.
Sampling weights were used to produce national estimates that are representative of the civilian noninstitutionalized U.S. population aged 18 and over (9). Point estimates and statistical tests were calculated using SUDAAN software version 11.0 (RTI International, Research Triangle Park, N.C.) to account for the complex sample design of NHIS. Calculations excluded persons with unknown information. Sensitivity analyses were conducted to examine if the observed disparities with non-Hispanic white men differed for non-Hispanic black men relative to Hispanic men. No significant differences were observed, so estimates for non-Hispanic white men were compared with pooled estimates for non-Hispanic black and Hispanic men. Estimates reported for all men (“all races and ethnicities”) include men with races and ethnicities other than non-Hispanic white, non-Hispanic black, and Hispanic. All comparisons were evaluated for statistical significance at the 0.05 level using two-sided tests.
Analyses of treatment use did not include the 4.6% of men who took medication for anxiety or depression but did not experience these feelings daily, perhaps as a result. The prevalence of medication use in the absence of daily feelings was lower for men of color (2.7%) relative to non-Hispanic white men (5.6%), and this difference did not vary by age or health insurance coverage status. Therefore, if the analyses in this report had included these men, treatment rates generally would have been higher, but all observed racial and ethnic differences would still be significant and the conclusions would not have changed.
About the authors
Stephen J. Blumberg, Tainya C. Clarke, and Debra L. Blackwell are with CDC’s National Center for Health Statistics, Division of Health Interview Statistics.
References
- Alegría M, Chatterji P, Wells K, Cao Z, Chen CN, Takeuchi D, et al. Disparity in depression treatment among racial and ethnic minority populations in the United States. Psychiatr Serv 59(11):1264–72. 2008.
- Broman CL. Race differences in the receipt of mental health services among young adults. Psychol Serv 9(1):38–48. 2012.
- HHS. Mental health: Culture, race, and ethnicity—A supplement to mental health: A report of the Surgeon General. Washington, DC. 2001.
- HHS. Mental health: A report of the Surgeon General. Washington, DC. 1999.
- Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry 62(6):593–602. 2005.
- Weissman J, Pratt LA, Miller EA, Parker JD. Serious psychological distress among adults: United States, 2009–2013. NCHS data brief, no 203. Hyattsville, MD: National Center for Health Statistics. 2015.
- Pratt LA, Brody DJ. Depression in the U.S. household population, 2009–2012. NCHS data brief, no 172. Hyattsville, MD: National Center for Health Statistics. 2014.
- Thompson VLS, Bazile A, Akbar M. African Americans’ perceptions of psychotherapy and psychotherapists. Professional psychology: Research and practice 35(1):19–26. 2004.
-
Parsons VL, Moriarity C, Jonas K, et al. Design and estimation for the National Health Interview Survey, 2006–2015. National Center for Health Statistics. Vital Health Stat 2(165). 2014.
Suggested citation
Blumberg SJ, Clarke TC, Blackwell DL. Racial and ethnic disparities in men’s use of mental health treatments. NCHS data brief, no 206. Hyattsville, MD: National Center for Health Statistics. 2015.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Charles J. Rothwell, M.S., M.B.A., Director
Nathaniel Schenker, Ph.D., Deputy Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Division of Health Care Statistics
Marcie L. Cynamon, Acting Director
- Page last reviewed: November 6, 2015
- Page last updated: June 11, 2015
- Content source: