

Cardiorespiratory Fitness Levels Among U.S. Youth Aged 12–15 Years: United States, 1999–2004 and 2012
 ShareCompartir
ShareCompartir
NCHS Data Brief No.153, May 2014
On This Page
- Key findings
- One-half of boys and about one-third of girls aged 12–15 years had adequate levels of cardiorespiratory fitness.
- The percentage of youth aged 12–15 who had adequate levels of cardiorespiratory fitness did not differ by race and Hispanic origin or family income-to-poverty ratio.
- A higher percentage of normal weight youth had adequate levels of cardiorespiratory fitness compared with overweight or obese youth.
- The percentage of youth aged 12–15 who had adequate levels of cardiorespiratory fitness decreased from 52.4% in 1999–2000 to 42.2% in 2012.
- Summary
- Definitions
- Data sources and methods
- About the authors
- References
- Suggested citation
PDF Version (423 KB)
Jaime Gahche, M.P.H.; Tala Fakhouri, Ph.D., M.P.H.; Dianna D. Carroll, Ph.D.; Vicki L. Burt, Sc.M., R.N.; Chia-Yih Wang, Ph.D.; and Janet E. Fulton, Ph.D.
Key findings
Data from the National Health and Nutrition Examination Survey (NHANES), 1999–2004 and the NHANES National Youth Fitness Survey, 2012
- In 2012, about 42% of U.S. youth aged 12–15 years had adequate levels of cardiorespiratory fitness.
- The percentage of youth who had adequate levels of cardiorespiratory fitness did not differ by race and Hispanic origin, or by family income-to-poverty ratio.
- The percentage of youth who had adequate levels of cardiorespiratory fitness decreased as weight status increased.
- The percentage of youth aged 12–15 who had adequate levels of cardiorespiratory fitness decreased from 52.4% in 1999–2000 to 42.2% in 2012.
Physical fitness has been defined as “a set of attributes that people have or achieve that relates to the ability to perform physical activity” (1). Cardiorespiratory fitness is one component of physical fitness and is defined as the “ability of the circulatory and respiratory systems to supply fuel during sustained physical activity and to eliminate fatigue products after supplying fuel” (1). Cardiorespiratory fitness is most often measured by maximal oxygen uptake (VO2max), which is the maximum capacity of the body to transport and use oxygen during physical activity (2). This report presents the most recent national data on the percentage of youth who had adequate levels of cardiorespiratory fitness. Adequate levels of cardiorespiratory fitness are based on standards that are age- and sex-specific and established based on how fit children need to be for good health.
Keywords: exercise testing, National Health and Nutrition Examination Survey, National Youth Fitness Survey
One-half of boys and about one-third of girls aged 12–15 years had adequate levels of cardiorespiratory fitness.
- Overall, 42.2% of youth aged 12–15 years had adequate levels of cardiorespiratory fitness in 2012 (Figure 1).
- A higher percentage of boys (50.2%) aged 12–15 had adequate levels of cardiorespiratory fitness compared with girls of the same age (33.8%).
- A similar pattern between age groups was observed for youth aged 12–13 and 14–15. For both age groups, a higher percentage of boys than girls had adequate levels of cardiorespiratory fitness.
- There was no significant difference between the younger and older age groups, for girls or boys, in the percentage of those who had adequate levels of cardiorespiratory fitness.
Figure 1. Percentage of youth aged 12–15 who had adequate levels of cardiorespiratory fitness, by sex and age group: United States, 2012
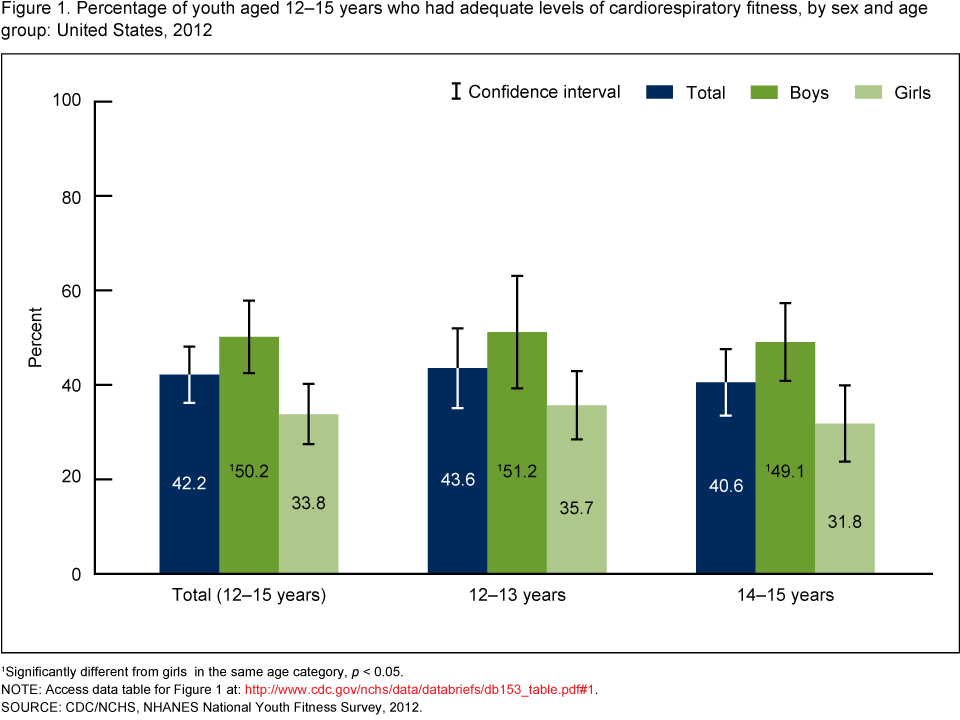
1Significantly different from girls in the same age category, p < 0.05.
NOTE: Access data table for Figure 1 [PDF - 125 KB].
SOURCE: CDC/NCHS, NHANES National Youth Fitness Survey, 2012.
The percentage of youth aged 12–15 who had adequate levels of cardiorespiratory fitness did not differ by race and Hispanic origin or family income-to-poverty ratio.
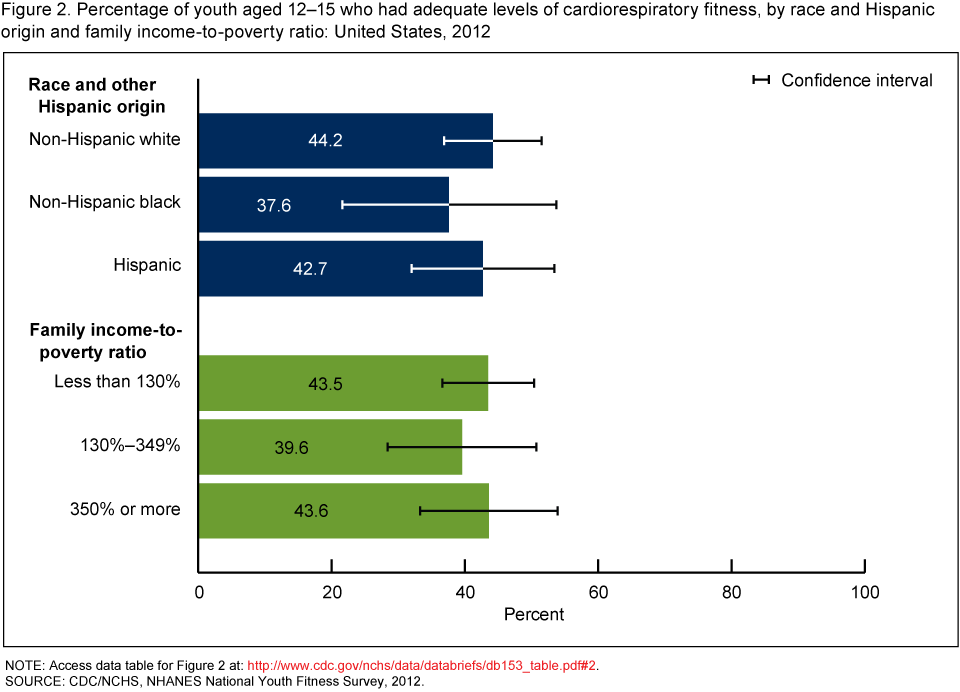
- There was no difference in the percentage who had adequate levels of cardiorespiratory fitness among non-Hispanic white, non-Hispanic black, and Hispanic youth (Figure 2).
- There was no statistically significant difference in the percentage of youth who had adequate levels of cardiorespiratory fitness among youth in families with incomes less than 130% of the federal poverty guidelines (43.5%), 130%–349% of the federal poverty guidelines (39.6%), or 350% or more of the federal poverty guidelines (43.6%).
Figure 2. Percentage of youth aged 12–15 who had adequate levels of cardiorespiratory fitness, by race and Hispanic origin and family income-to-poverty ratio: United States, 2012
NOTE: Access data table for Figure 2 [PDF - 125 KB].
SOURCE: CDC/NCHS, NHANES National Youth Fitness Survey, 2012.
A higher percentage of normal weight youth had adequate levels of cardiorespiratory fitness compared with overweight or obese youth.
- Among all youth aged 12–15, a higher percentage of normal weight youth (54.1%) had adequate levels of cardiorespiratory fitness compared with overweight (29.9%) or obese (20.0%) youth (Figure 3).
Figure 3. Percentage of youth aged 12–15 who had adequate levels of cardiorespiratory fitness, by weight status: United States, 2012
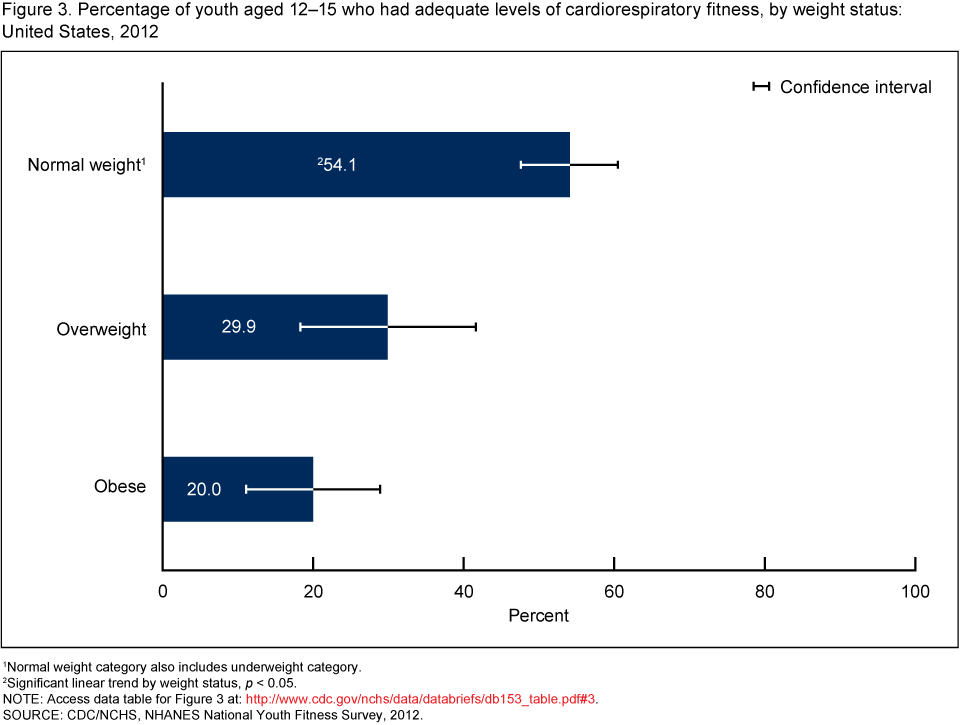
1Normal weight category also includes underweight category.
2Significant linear trend by weight status, p < 0.05.
NOTE: Access data table for Figure 3 [PDF - 125 KB].
SOURCE: CDC/NCHS, NHANES National Youth Fitness Survey, 2012.
The percentage of youth aged 12–15 who had adequate levels of cardiorespiratory fitness decreased from 52.4% in 1999–2000 to 42.2% in 2012.
- Overall, 52.4% of youth in 1999–2000, 51.1% in 2001–2002, 47.6% in 2003–2004, and 42.2% in 2012 had adequate levels of cardiorespiratory fitness (Figure 4).
- A higher percentage of boys than girls had adequate levels of cardiorespiratory fitness for all periods.
- The percentage of boys who had adequate cardiorespiratory fitness levels decreased significantly from 64.8% in 1999–2000 to 50.2% in 2012. The percentage of girls decreased from 40.5% in 1999–2000 to 33.8% in 2012, however, this was not significant.
Figure 4. Percentage of youth aged 12–15 who had adequate levels of cardiorespiratory fitness, by sex and survey period: United States, 1999–2004 and 2012
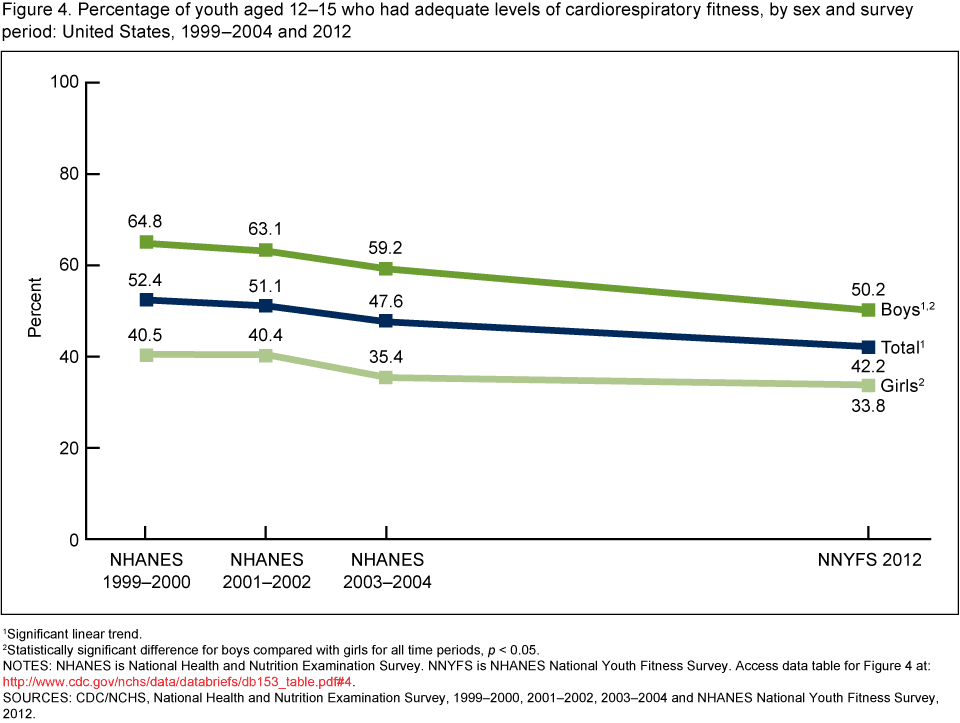
1Significant linear trend.
2Statistically significant difference for boys compared with girls for all time periods, p < 0.05.
NOTES: NHANES is National Health and Nutrition Examination Survey. NNYFS is NHANES National Youth Fitness Survey. Access data table for Figure 4 [PDF - 125 KB].
SOURCES: CDC/NCHS, National Health and Nutrition Examination Survey, 1999–2000, 2001–2002, 2003–2004 and NHANES National Youth Fitness Survey, 2012.
Summary
This report presents the percentage of U.S. youth aged 12–15 who had adequate levels of cardiorespiratory fitness, by sex, age group, race and Hispanic origin, family income-to-poverty ratio, weight status, and across time. The findings indicate that one-half of boys and one-third of girls aged 12–15 had adequate levels of cardiorespiratory fitness. No significant differences were found in the percentage of youth having adequate levels of cardiorespiratory fitness by race and Hispanic origin, or by family income-to-poverty ratio. Compared with normal weight youth, a smaller percentage of overweight and obese youth had adequate levels of cardiorespiratory fitness. About one in five adolescents aged 12–19 in the United States is obese (3).
The percentage of youth who had adequate levels of cardiorespiratory fitness was compared across four survey periods: NHANES 1999–2000, 2001–2002, 2003–2004, and NNYFS 2012. The findings indicate the percentage of youth with adequate cardiorespiratory fitness decreased from 52.4% in 1999–2000 to 42.2% in 2012.
Definitions
Adequate Cardiorespiratory Fitness: Refers to the “Healthy Fitness Zone” threshold established and developed by the Cooper Institute’s fitness assessment, FITNESSGRAM, a youth physical fitness testing program that has been used by schools and school districts nationally. The “Healthy Fitness Zone” threshold is age- and sex-specific. It was established by comparing youth cardiorespiratory fitness levels with measures of health in a nationally representative sample (NHANES 1999–2002) aged 12–18 (4).
Family income-to-poverty ratio (FIPR): Calculated by dividing family income by a poverty measure specific for family size. The U.S. Department of Health and Human Services’ poverty guidelines were used as the poverty measure to calculate FIPR (5). FIPR accounts for inflation. Income eligibility for participation in the Supplemental Nutrition Assistance Program (SNAP) is 130% of the FIPR (< 130% FIPR) (6). Larger FIPRs indicate greater income.
Weight status: Categories were based on the Centers for Disease Control and Prevention’s (CDC) sex-specific 2000 body mass index (BMI)-for-age growth charts for the United States (7). The three categories were underweight or normal weight (a BMI-for-age less than the 85th percentile), overweight (a BMI-for-age ranging from the 85th to less than the 95th percentile), and obese (a BMI-for-age greater than or equal to the 95th percentile).
Data sources and methods
NHANES 1999–2000, 2001–2002, and 2003–2004 and NNYFS 2012 were used for the analyses presented in this report, and all data are publicly available on the NHANES website. Both NHANES and NNYFS are conducted by CDC’s National Center for Health Statistics (NCHS) to monitor the health and nutritional status of the U.S. population. Both of these population-based surveys use a complex, stratified, multistage probability cluster sampling design. NHANES data collection is based on a nationally representative sample covering all ages of the civilian noninstitutionalized United States (8). NNYFS was a 1-year survey conducted in 2012 to obtain data on the physical activity and fitness levels of children and adolescents aged 3–15 years in the United States (9). This survey was conducted in conjunction with the 2012 NHANES and the survey design was based on the design for NHANES, with the NNYFS sample selected from an independent sample of dwelling units within the segments selected for NHANES. In both NHANES and NNYFS, participants received an interview at their homes and then a physical fitness examination in a specially equipped mobile examination center.
Cardiorespiratory fitness was measured using a submaximal treadmill test. This test was conducted using the same protocol for all survey periods (10,11). Participants were assigned to one of five treadmill test protocols varying in grade and speed based on sex, age, BMI, and level of self-reported physical activity. The goal of each protocol was to elicit a heart rate that was approximately 75% of the age-predicted maximal heart rate. Heart rates after each of the two exercise stages were then used in an equation to estimate VO2max. The percentage of youth who had adequate levels of cardiorespiratory fitness was then determined based on the thresholds set by The Cooper Institute (12).
Self-reported race and Hispanic origin groups as defined in NHANES and used in the analysis were non-Hispanic white, non-Hispanic black, Hispanic, and ‘‘other.’’ Following NCHS recommendations, the ‘‘other’’ racial or ethnic group was included in the estimates for the total sample, but was not presented separately as a group.
All analyses used the examination sample weights, which account for unequal probabilities of selection, person-level nonresponse, and a poststratification adjustment to the estimated U.S. population. Taylor series linearization was used to calculate standard errors. Confidence limits of 95% were constructed using the Wald method. Differences between groups were assessed using a univariate t statistic at the p < 0.05 significance level with the appropriate degrees of freedom. To test for linear trends, the null hypothesis of a nonlinear trend was examined using orthogonal polynomials. Statistical analyses were conducted using SAS version 9.3 (SAS Institute, Inc., Cary, N.C.) and SUDAAN version 11.0 (RTI International, Research Triangle Park, N.C.).
About the authors
Jaime Gahche, Tala Fakhouri, Vicki L. Burt, and Chia-Yih Wang are with CDC’s National Center for Health Statistics, Division of Health and Nutrition Examination Surveys. Dianna D. Carroll is with CDC’s National Center on Birth Defects and Developmental Disabilities, and Janet E. Fulton is with CDC’s National Center for Chronic Disease Prevention and Health Promotion.
References
- Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep 100(2):126–31. 1985.
- Gordon RS, Franklin KL, Baker JS, Davies B. Determination of aerobic work and power on a rope-braked cycle ergometer by direct measurement. Appl Physiol Nutr Metab 31(4):392–7. 2006.
- Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of childhood and adult obesity in the United States, 2011–2012. JAMA 311(8):806–14. 2014.
- Welk GJ, Laurson KR, Eisenmann JC, Cureton KJ. Development of youth aerobic-capacity standards using receiver operating characteristic curves. Am J Prev Med 41(4 Suppl 2):S111–6. 2011.
- U.S. Department of Health and Human Services. Poverty guidelines, research, and measurement. [Accessed March 25, 2014].
- U.S. Department of Agriculture. Supplemental Nutrition Assistance Program (SNAP): Eligibility. [Accessed March 28, 2014].
- Ogden CL, Flegal KM. Changes in terminology for childhood overweight and obesity. National health statistics reports; no 25. Hyattsville, MD: National Center for Health Statistics. 2010.
- Zipf G, Chiappa M, Porter KS, et al. National Health and Nutrition Examination Survey: Plan and operations, 1999–2010. National Center for Health Statistics. Vital Health Stat 1(56). 2013.
- Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey National Youth Fitness Survey (NNYFS), 2012. Hyattsville, MD: National Center for Health Statistics. 2013. [Accessed November 5, 2013].
- Centers for Disease Control and Prevention. National Youth Fitness Survey (NYFS) Treadmill Examination Manual. Hyattsville, MD: National Center for Health Statistics. 2013. [Accessed November 5, 2013].
- Centers for Disease Control and Prevention. Cardiovascular Fitness Procedures Manual. Hyattsville, MD: National Center for Health Statistics. 2004. [Accessed November 5, 2013].
- Meredith MD, Welk GJ. Fitnessgram & Activitygram Test Administration Manual, Updated 4th Edition. Dallas, TX: The Cooper Institute. 2010.
Suggested citation
Gahche J, Fakhouri T, Carroll DD, et al. Cardiorespiratory fitness levels among U.S. youth aged 12–15 years: United States, 1999–2004 and 2012. NCHS data brief, no 153. Hyattsville, MD: National Center for Health Statistics. 2014.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Charles J. Rothwell, M.S., M.B.A., Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Division of Health and Nutrition Examination Surveys
Kathryn S. Porter, M.D., M.S., Director
- Page last reviewed: November 6, 2015
- Page last updated: May 28, 2014
- Content source: