

Psychotropic Medication Use Among Adolescents: United States, 2005–2010
 ShareCompartir
ShareCompartir
NCHS Data Brief No. 135, December 2013
On This Page
- Key findings
- More than 6.0% of adolescents reported the use of psychotropic medications.
- Male and female adolescents differed in their use of psychotropic medications.
- Non-Hispanic white adolescents were more likely to report the use of psychotropic medications.
- About one-half of adolescents reporting any psychotropic medication use had seen a mental health professional in the past year.
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
PDF Version (481 KB)
Bruce S. Jonas, Sc.M., Ph.D.; Qiuping Gu, M.D., Ph.D.; and Juan R. Albertorio-Diaz, M.A.
Key findings
Data from the National Health and Nutrition Examination Survey
- Approximately 6.0% of U.S. adolescents aged 12–19 reported psychotropic drug use in the past month.
- The use of antidepressants (3.2%) and attention deficit hyperactive disorder (ADHD) drugs (3.2%) was highest, followed by antipsychotics (1.0%); anxiolytics, sedatives, and hypnotics (0.5%); and antimanics (0.2%).
- Males (4.2%) were more likely than females (2.2%) to use ADHD drugs. Females (4.5%) were more likely than males (2.0%) to use antidepressants.
- Psychotropic drug use was higher among non-Hispanic white (8.2%) adolescents than non-Hispanic black (3.1%) and Mexican-American (2.9%) adolescents.
- About one-half of U.S. adolescents using psychotropic drugs in the past month had seen a mental health professional in the past year (53.3%).
Prior studies have shown an increase in psychotropic medication use among adolescents (1–6). However, most studies were based on clinical samples or high-risk populations. This report provides the estimate of any psychotropic medication use in the past month among U.S. noninstitutionalized adolescents aged 12–19 during 2005–2010, using National Health and Nutrition Examination Survey (NHANES) data. Psychotropic medication is a type of drug used to treat clinical psychiatric symptoms or mental disorders (7). Specific psychotropic drug types addressed are antidepressants; medications for attention deficit hyperactive disorder (ADHD); anxiolytics, sedatives, and hypnotics (ASH); antimanics; and antipsychotics. Adolescents using psychotropic drugs are further examined by sex, race and Hispanic origin, and mental health professional consultation.
Keywords: National Health and Nutrition Examination Survey, ADHD drugs, antidepressants, prescription
More than 6.0% of adolescents reported the use of psychotropic medications.
Figure 1. Percentage of adolescents aged 12–19 taking psychotropic medications in the past month, overall and by drug class: United States, 2005–2010

* Does not meet standards of reliability or precision; relative standard error greater than 30%.
NOTES: ADHD is attention deficit hyperactive disorder. ASH is anxiolytics, sedatives, and hypnotics.
SOURCE: CDC/NCHS, National Health and Nutrition Examination Survey, 2005–2010.
- A total of 6.3% of the population aged 12–19 reported any psychotropic medication use in the past month. This included 4.5% taking only one psychotropic medication, and 1.8% taking two or more psychotropic medications (Figure 1).
- Antidepressants and ADHD medications (3.2% each) were the most frequent psychotropic drugs used among adolescents.
- One percent of adolescents reported the use of antipsychotic medications.
- Less than 1.0% of the U.S. adolescent population reported the use of prescribed ASH or antimanics.
Male and female adolescents differed in their use of psychotropic medications.
Figure 2. Psychotropic medication use in the past month among adolescents, by sex: United States, 2005–2010
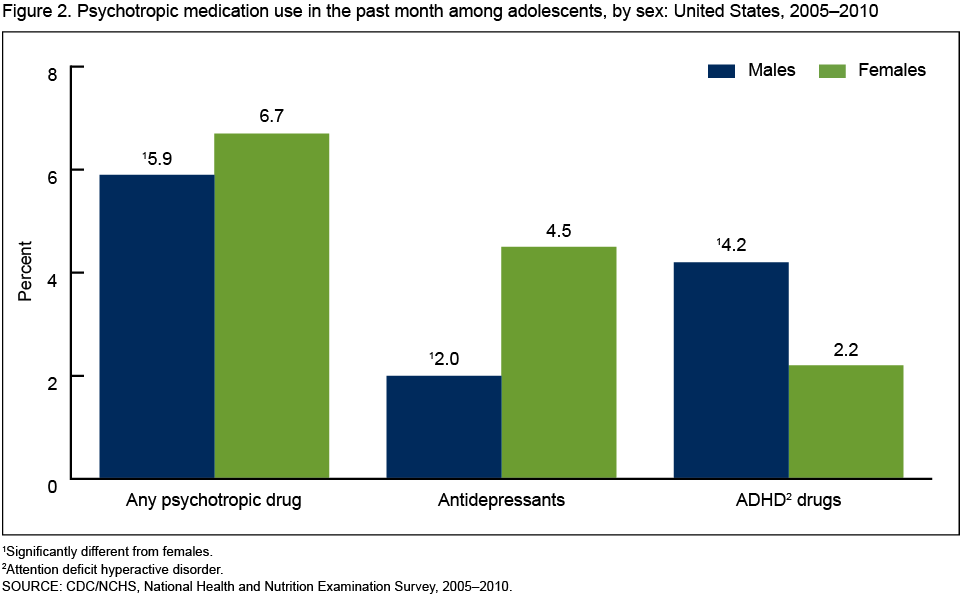
1Significantly different from females.
2Attention deficit hyperactive disorder.
SOURCE: CDC/NCHS, National Health and Nutrition Examination Survey, 2005–2010.
- Overall, females (6.7%) were more likely than males (5.9%) to report the use of any psychotropic medications in the past month (Figure 2).
- Females (4.5%) were more likely than males (2.0%) to report the use of antidepressants in the past month.
- In contrast, males (4.2%) were more likely than females (2.2%) to report using ADHD medications in the past month.
Non-Hispanic white adolescents were more likely to report the use of psychotropic medications.
Figure 3. Psychotropic medication use among adolescents, by race and Hispanic origin: United States, 2005–2010
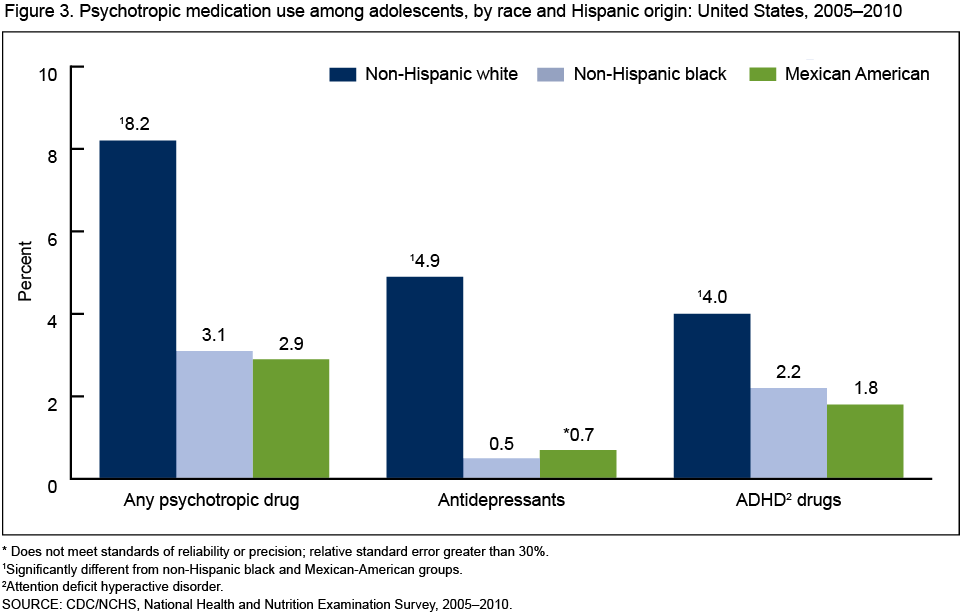
* Does not meet standards of reliability or precision; relative standard error greater than 30%.
1Significantly different from non-Hispanic black and Mexican-American groups.
2Attention deficit hyperactive disorder.
SOURCE: CDC/NCHS, National Health and Nutrition Examination Survey, 2005–2010.
- More than 8.0% of non-Hispanic white adolescents reported using psychotropic medications, compared with 3.1% of non-Hispanic black and 2.9% of Mexican-American adolescents (Figure 3).
- Non-Hispanic white adolescents (4.9%) were more likely than non-Hispanic black (0.5%) and Mexican-American (0.7%) adolescents to report antidepressant medication use.
- Non-Hispanic white adolescents (4.0%) were more likely than non-Hispanic black (2.2%) and Mexican-American (1.8%) adolescents to report the use of medications for ADHD.
- No significant difference was observed between non-Hispanic black and Mexican-American adolescents in the use of any psychotropic medications, antidepressants, or ADHD drugs.
About one-half of adolescents reporting any psychotropic medication use had seen a mental health professional in the past year.
Figure 4. Percentage of adolescents aged 12–19 taking psychotropic medications in the past month who had seen a mental health professional in the past year: United States, 2005–2010
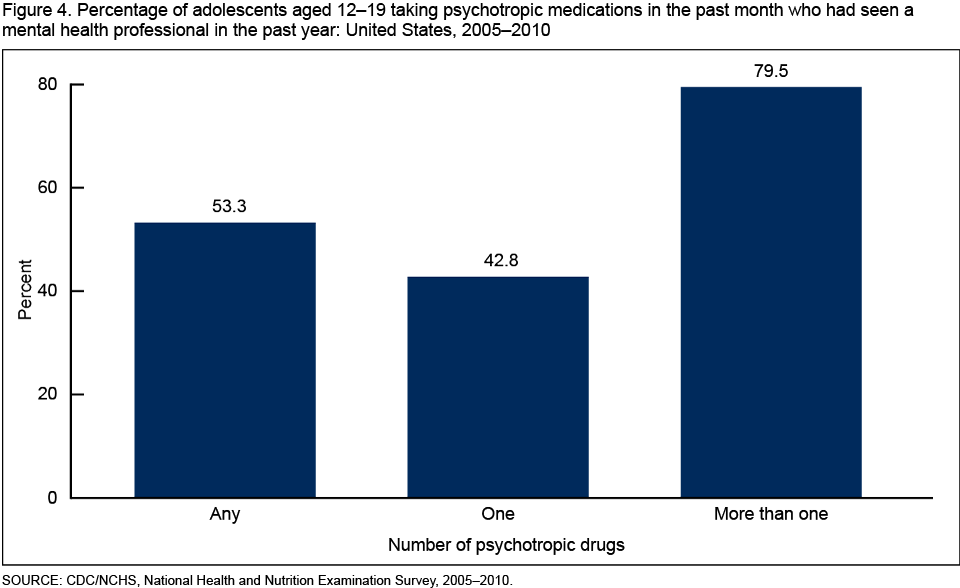
SOURCE: CDC/NCHS, National Health and Nutrition Examination Survey, 2005–2010.
- Approximately 43.0% of adolescents taking one psychotropic medication had seen a mental health professional in the past year (42.8%) (Figure 4).
- Almost 80.0% of adolescents taking two or more psychotropic medications had seen a mental health professional in the past year (79.5%).
Summary
During 2005–2010, 6.3% of the U.S. adolescent population aged 12–19 reported any psychotropic medication use in the past month. The percentages of psychotropic medication use by drug class were 3.2% for antidepressants, 3.2% for ADHD drugs, 1.0% for antipsychotics, 0.5% for ASH, and 0.2% for antimanics. Males were more likely than females to report ADHD medication use, while females were more likely than males to report antidepressant use. Non-Hispanic white adolescents reported higher antidepressant use than either non-Hispanic black or Mexican-American adolescents. A similar pattern was observed for ADHD medication use. Approximately one-half of the adolescent population reporting any psychotropic medication use in the past month had seen a mental health professional in the past year.
Depression and ADHD are the most common mental health disorders among adolescents. About 4.3% of adolescents aged 12–17 experienced depression in any 2-week period during 2005–2006 (8). Approximately 9.0% of children aged 5–17 had ever been diagnosed with ADHD during 2007–2009 (9). Treatment options other than prescription medication are available for depression, ADHD, and other mental health disorders, including psychosocial treatment and dietary management (10,11), both of which were unavailable for analysis in this report.
Definitions
Prescribed medication use: During an in-person home interview, NHANES participants are asked: "In the past 30 days, have you used or taken medication for which a prescription is needed?" Respondents who reply "Yes" are further asked to present to the interviewer the container of all prescribed medications mentioned. For each drug reported, the interviewer records the product's complete name from the container. To standardize the medication nomenclature, all reported medication names are converted to standard generic names.
Psychotropic medication: Prescription drugs are classified according to Cerner Multum's Lexicon (12) three-level nested therapeutic classification scheme. Antidepressants, antipsychotics, and ASH are identified using the second level of drug category codes 249, 251, and 67, respectively. Antimanics include lithium, carbamazepine, and valproic acid. Prescription drugs for ADHD (7,10) include amphetamine, atomoxetine, dexmethylphenidate, dextroamphetamine, guanfacine, lisdexamphetamine, methamphetamine, and methylphenidate. Respondents who reported using any of these five drug classes were classified as a psychotropic medication user. Adolescents who reported using more than one psychotropic drug were defined as multiple psychotropic medication users.
Contact with a mental health professional: Contact was based on the following survey question: "During the past 12 months, have you seen or talked to a mental health professional such as a psychologist, psychiatrist, psychiatric nurse, or clinical social worker about your health?"
Data source and methods
NHANES is a continuous, multipurpose cross-sectional survey of the civilian noninstitutionalized U.S. population designed to assess the overall health and nutrition of the American population in the contiguous states.
The sample design includes oversampling to obtain reliable estimates of health and nutritional measures for population subgroups. During 2005–2006, adolescent, elderly, low-income, black, and Mexican-American persons were oversampled. During 2007–2010, adolescents were no longer oversampled. In addition, Hispanic persons, rather than Mexican-American persons, were oversampled.
This study examines the percentage of prescription psychotropic medication use among adolescents aged 12–19. For the sample age group 12–15, a proxy respondent, usually one of the child's parents, answered the questions in the household interview. Percentage estimates of psychotropic medication use based on NHANES data come from a nationally representative household sample. As such, they are likely conservative estimates, because they exclude higher-risk populations such as the homeless and those in correctional facilities and inpatient treatment facilities.
NHANES consists of an interview conducted in the participant's home and a standardized physical examination performed in a mobile examination center. This report is based on interview data conducted at the respondent's home. Therefore, interview sample weights, which account for the differential probabilities of selection, nonresponse, and noncoverage, are used for the analysis presented here.
Robust standard errors of the percentages are estimated using Taylor series linearization, a method that takes into consideration the sample weights and sample design. All statistical tests are two-sided using p < 0.05 as the level of significance. All reported comparisons are statistically significant unless otherwise indicated. Statistical analyses were conducted using SAS version 9.3 (SAS Institute, Cary, N.C.) and SUDAAN version 10.0 (RTI International, Research Triangle Park, N.C.).
About the authors
Bruce Jonas is with the Centers for Disease Control and Prevention's National Center for Health Statistics (CDC/NCHS), Office of Analysis and Epidemiology; Qiuping Gu is with CDC/NCHS, Division of Health and Nutrition Examination Surveys; and Juan Albertorio-Diaz is with CDC/NCHS, International Statistics Program.
References
- Steffenak AK, Wilde-Larsson B, Nordström G, Skurtveit S, Hartz I. Increase in psychotropic drug use between 2006 and 2010 among adolescents in Norway: A nationwide prescription database study. Clin Epidemiol 4:225–31. 2012.
- Zito JM, Safer DJ, DosReis S, Gardner JF, Magder L, Soeken K, et al. Psychotropic practice patterns for youth: A 10-year perspective. Arch Pediatr Adolesc Med 157(1): 17–25. 2003.
- Zito JM, Tobi H, de Jong-van den Berg LT, Fegert JM, Safer DJ, Janhsen K, et al. Antidepressant prevalence for youths: A multi-national comparison. Pharmacoepidemiol Drug Saf 15(11):793–8. 2006.
- Fegert JM, Kölch M, Zito JM, Glaeske G, Janhsen K. Antidepressant use in children and adolescents in Germany. J Child Adolesc Psychopharmacol 16(1–2):197–206. 2006.
- Zoëga H, Baldursson G, Hrafnkelsson B, Almarsdóttir AB, Valdimarsdóttir U, Halldórsson M. Psychotropic drug use among Icelandic children: A nationwide population-based study. J Child Adolesc Psychopharmacol 19(6):757–64. 2009.
- Hsia Y, Maclennan K. Rise in psychotropic drug prescribing in children and adolescents during 1992–2001: A population-based study in the UK. Eur J Epidemiol 24(4):211–6. 2009.
- National Institute of Mental Health. Mental health medications. NIH publication no. 12–3929. 2010.
- Pratt LA, Brody DJ. Depression in the United States household population, 2005–2006. NCHS data brief, no 7. Hyattsville, MD: National Center for Health Statistics. 2008.
- Akinbami LJ, Liu X, Pastor PN, Reuben CA. Attention deficit hyperactivity disorder among children aged 5–17 years in the United States, 1998–2009. NCHS data brief, no 70. Hyattsville, MD: National Center for Health Statistics. 2011.
- Ravindran AV, da Silva TL. Complementary and alternative therapies as add-on to pharmacotherapy for mood and anxiety disorders: A systematic review. J Affect Disord 150(3):707–19. 2013.
- Qureshi NA, Al-Bedah AM. Mood disorders and complementary and alternative medicine: A literature review. Neuropsychiatr Dis Treat 9:639–58. 2013.
- National Center for Health Statistics. National Health and Nutrition Examination Survey, 1988–2010 data documentation, codebook, and frequencies: Prescription medications–drug information (RXQ_DRUG). 2012.
Suggested citation
Jonas BS, Gu Q, Albertorio-Diaz JR. Psychotropic medication use among adolescents: United States, 2005–2010. NCHS data brief, no 135. Hyattsville, MD: National Center for Health Statistics. 2013.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Charles J. Rothwell, M.S., Acting Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Office of Analysis and Epidemiology
Irma E. Arispe, Ph.D., Director
- Page last reviewed: November 6, 2015
- Page last updated: December 2, 2013
- Content source: