

Wait Time for Treatment in Hospital Emergency Departments: 2009
 ShareCompartir
ShareCompartir
NCHS Data Brief No. 102, August 2012
On This Page
- Key findings
- Has wait time for treatment in EDs increased?
- Does ED crowding affect wait time?
- How does hospital location and ED crowding affect wait time?
- How does ED visit volume and ED crowding affect wait time?
- Does patient acuity affect wait time for treatment in EDs?
- Does ED crowding affect wait time for treatment when patient acuity is controlled for?
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
PDF Version (793 KB)
Esther Hing, M.P.H., and Farida Bhuiya, M.P.H.
Key findings
- From 2003 through 2009, the mean wait time in U.S. emergency departments (EDs) increased 25%, from 46.5 minutes to 58.1 minutes.
- Mean wait times were longer in EDs that went on ambulance diversion or boarded admitted patients in hallways and in other spaces.
- Longer wait times were associated with EDs in urban areas (62.4 minutes), compared with nonurban areas (40.0 minutes).
- The mean wait time increased as annual ED visit volume increased; from 33.8 minutes in EDs with less than 20,000 annual visits, to 69.8 minutes in EDs with 50,000 or more annual visits.
- There was no difference in mean wait time for patients needing immediate or emergent care by ambulance diversion status, or by whether the ED boarded admitted patients while waiting for an inpatient bed.
From 1999 through 2009, the number of visits to emergency departments (EDs) increased 32%, from 102.8 million visits in 1999 to 136.1 million visits in 2009 (1,2). In some hospitals, increased ED visit volume has resulted in ED crowding and increased wait times for minor and sometimes serious problems, such as myocardial infarction (3–7). This report describes the recent trend in wait times for treatment in EDs, and focuses on how wait times for treatment varied by two ED crowding measures: ambulance diversions and boarding of admitted patients.
Keywords: emergency department crowding, ambulance diversion, boarding
Has wait time for treatment in EDs increased?
- Between 2003 and 2009, mean wait time to see a provider increased 25%, from 46.5 minutes to 58.1 minutes (Figure 1).
- Because wait time is highly skewed, that is, a small percentage (5%) of visits have very long wait times (greater than 3 hours), median wait time is less affected by the skewed distribution and provides an alternative way of describing ED wait time.
Figure 1. Mean and median emergency department wait time to see a provider: United States, 2003–2009
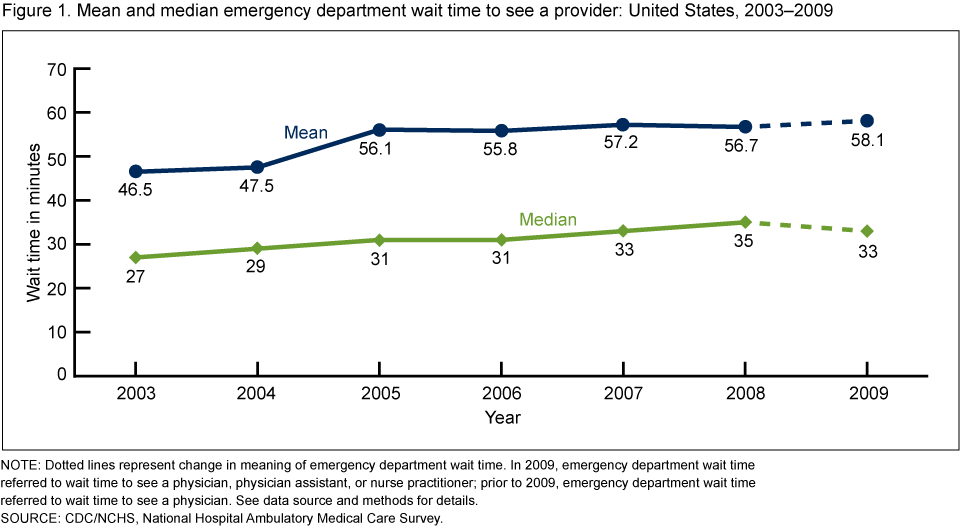
NOTE: Dotted lines represent change in meaning of emergency department wait time. In 2009, emergency department wait time referred to wait time to see a physician, physician assistant, or nurse practitioner; prior to 2009, emergency department wait time referred to wait time to see a physician. See data source and methods for details.
SOURCE: CDC/NCHS, National Hospital Ambulatory Medical Care Survey.
- Between 2003 and 2009, median time to see a provider increased 22%, from 27 minutes to 33 minutes.
Does ED crowding affect wait time?
- In 2009, 33% of ED visits occurred in EDs that reported they went on ambulance diversion at some time during the previous year; 40% of visits occurred in EDs that reported they did not go on ambulance diversion; and 27% of visits occurred in EDs that reported it was unknown whether the ED went on ambulance diversion (Figure 2).
- The average wait time to see an ED provider in EDs with ambulance diversions (64.3 minutes) was longer than in EDs with no diversions (48.7 minutes), but was similar to EDs for which diversions were unknown (65.2 minutes).
- In 2009, 78% of visits occurred in EDs that reported boarding admitted patients in hallways and in other spaces while waiting for an inpatient bed to become available.
- Wait time in EDs with any boarding was longer (61.3 minutes) than wait time in EDs with no boarding (44.1 minutes).
Figure 2. Mean wait time for treatment, by emergency department crowding measure: United States, 2009

1Significantly different from no diversion.
2Significantly different from no boarding.
SOURCE: CDC/NCHS, National Hospital Ambulatory Medical Care Survey.
How does hospital location and ED crowding affect wait time?
- Wait time in urban EDs (62.4 minutes) was significantly longer than in EDs outside of metropolitan areas (40.0 minutes) (Figure 3).
- The mean wait time among EDs reporting ambulance diversions was not significantly different in urban and nonurban hospitals (64.1 minutes compared with 68.4 minutes). The mean wait time in EDs with no ambulance diversions was longer among urban EDs (55.9 minutes) than among nonurban EDs (38.1 minutes).
- Among EDs that boarded admitted patients, the mean wait time was longer in urban EDs (64.3 minutes) than in nonurban EDs (42.9 minutes). The difference in mean wait time by hospital location among EDs that did not board was not statistically significant.
Figure 3. Mean wait time for treatment, by emergency department crowding measure and hospital location: United States, 2009
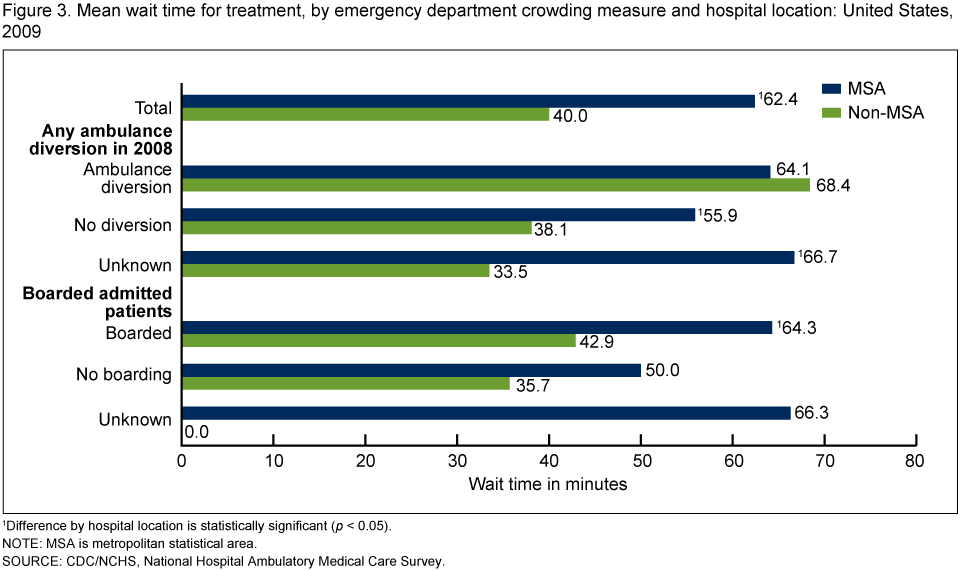
1Difference by hospital location is statistically significant (p < 0.05).
NOTE: MSA is metropolitan statistical area.
SOURCE: CDC/NCHS, National Hospital Ambulatory Medical Care Survey.
How does ED visit volume and ED crowding affect wait time?
- Mean wait time increased as the volume of annual ED visits increased; from 33.8 minutes in EDs with less than 20,000 annual visits, to 69.8 minutes in EDs with 50,000 or more annual visits (Figure 4).
- Mean wait time to see a health care provider increased as annual ED visit volume increased in each ambulance diversion category.
- The mean wait time in EDs that boarded patients increased as annual ED visit volume increased. Among EDs that did not board patients, EDs with less than 20,000 annual visits had shorter wait times than those with more than 20,000 annual visits; but there was no difference in wait times for EDs with 20,000–49,999 visits and those with 50,000 or more visits.
Figure 4. Mean wait time for treatment, by emergency department crowding measure and volume of annual emergency department visits: United States, 2009
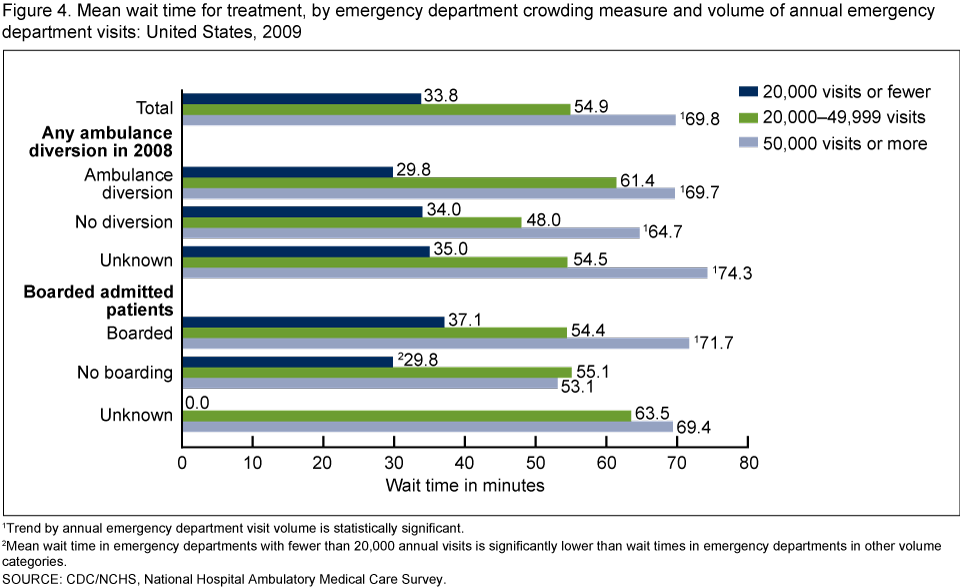
1Trend by annual emergency department visit volume is statistically significant.
2Mean wait time in emergency departments with fewer than 20,000 annual visits is significantly lower than wait times in emergency departments in other volume categories.
SOURCE: CDC/NCHS, National Hospital Ambulatory Medical Care Survey.
Does patient acuity affect wait time for treatment in EDs?
- Two percent of ED patients were triaged as needing to be seen in less than 1 minute (immediate); 10% were triaged as needing to be seen within 1–14 minutes (emergent); 41% were triaged as needing to be seen within 15–60 minutes (urgent); 35% were triaged as needing to be seen within 1–2 hours (semiurgent); and 7% of patients were triaged as needing to be seen between 2 and 24 hours (nonurgent). No triage system was used for the remaining 4% of patients (Figure 5).
- Mean wait times for patients triaged as immediate (28.9 minutes) and those with no triage system (38.2 minutes) were shorter than mean wait times for patients triaged as emergent (51.2 minutes), urgent (63.3 minutes), semiurgent (58.7 minutes), and nonurgent (53.5 minutes).
Figure 5. Mean emergency department wait time for treatment, by urgency of patient care: United States, 2009

1Difference with immediate care is statistically significant (p < 0.05).
2Difference with no triage is statistically significant (p < 0.05).
SOURCE: CDC/NCHS, National Hospital Ambulatory Medical Care Survey.
Does ED crowding affect wait time for treatment when patient acuity is controlled for?
- There were no differences in mean wait times for ED patients triaged as immediate or emergent between EDs that went on diversion and EDs that did not go on diversion (Figure 6). Similarly, there were no differences in wait times for ED patients triaged as immediate or emergent by whether the ED boarded any admitted patients.
- Patients triaged as urgent, semiurgent, or nonurgent, and patients that had no triage, had longer wait times in EDs that went on diversion compared with EDs that did not go on diversion.
- Patients triaged as urgent, semiurgent, or nonurgent, and patients that had no triage, had longer wait times in EDs that boarded any admitted patients compared with EDs that did not board any admitted patients.
Figure 6. Mean wait time for treatment, by urgency of patient care and whether emergency department experienced ambulance diversions or boarding: United States, 2009
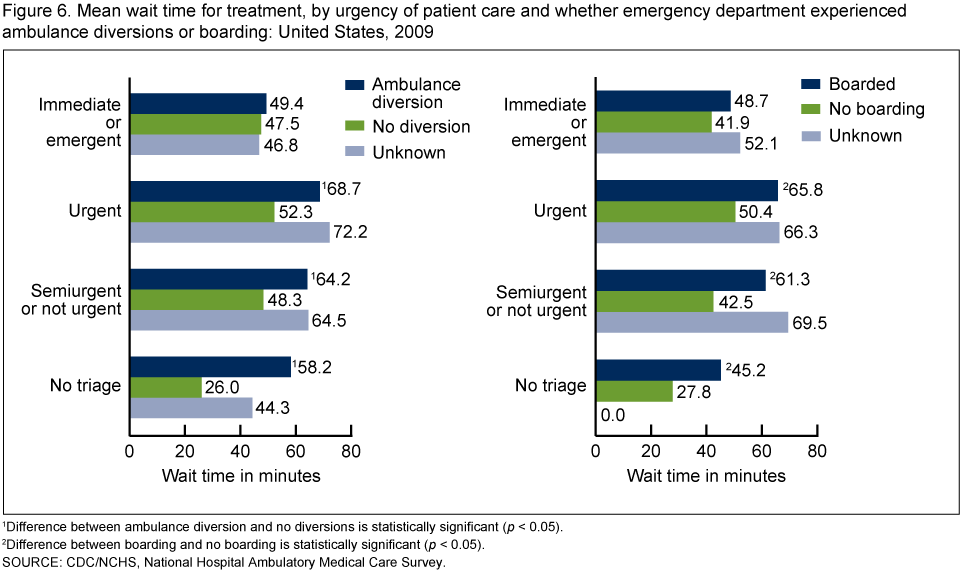
1Difference between ambulance diversion and no diversions is statistically significant (p < 0.05).
2Difference between boarding and no boarding is statistically significant (p < 0.05).
SOURCE: CDC/NCHS, National Hospital Ambulatory Medical Care Survey.
Summary
Mean wait time to see a health care provider in EDs increased from 2003 through 2009. Consistent with previous research, longer wait time for treatment was associated with urban ED locations (inside metropolitan statistical areas) and with increased annual ED visit volume (6).
In 2009, EDs with any ambulance diversion during the previous year were associated with longer wait times, compared with EDs without ambulance diversions. EDs that boarded admitted patients inside the ED, in observation units, or outside the ED (in hallways) were also associated with longer wait times compared with EDs that did not board. In this analysis, mean wait times for treatment did not differ among urban EDs that went on ambulance diversion during the previous year, but mean wait times were longer among urban EDs and nonurban EDs with no ambulance diversions and with unknown ambulance diversion status. Among EDs that boarded admitted patients (either inside or outside ED spaces), mean wait times were longer in EDs with annual visit volumes of 20,000 or more.
The mean wait time in EDs with unknown ambulance diversion status was similar to the wait time in EDs that went on ambulance diversion. The mean wait time in EDs for which boarding was unknown was also similar to the mean wait time in EDs that boarded patients inside or outside the ED. Figures 3 and 4 further indicate that ED visits missing information on ambulance diversions were all located in urban EDs and in EDs with annual visit volumes of 20,000 or more. The long mean wait times for visits in EDs missing information on ambulance diversions, as well as the high percentage (71%) that also reported boarding admitted patients, suggest that these EDs may have been on ambulance diversion.
There was no difference in mean wait time for patients triaged as immediate or emergent between EDs that went on diversion compared with EDs that did not go on diversion. There was also no difference in wait time for patients triaged as immediate or emergent by whether the ED boarded patients.
This analysis indicates that EDs are continuing to experience pressure to treat more patients with fewer EDs and with fewer hospital beds. Patients not requiring immediate care have longer wait times in EDs experiencing crowding (i.e., went on ambulance diversion or boarded admitted patients while waiting for an inpatient bed).
Definitions
Emergency department crowding: An ED is considered crowded when inadequate resources to meet patient care demands lead to a reduction in the quality of care (8).
Ambulance diversion: An ambulance is diverted when hospitals request that ambulances bypass their ED and transport patients to other medical facilities (4).
Boarding: A patient remains in the ED after the decision to admit or transfer the patient has been made (e.g., because an inpatient bed elsewhere in the hospital is not yet available) (4).
Data source and methods
All estimates are from the National Hospital Ambulatory Medical Care Survey (NHAMCS), an annual nationally representative survey of visits to nonfederal, general, and short-stay hospital emergency and outpatient departments. ED visit response rate was 83% in 2009. More details about NHAMCS methodology are available (9).
In 2009, ED wait time data were reported for visits seen by a physician, physician assistant, or nurse practitioner (n = 30,904). Prior to 2009, only wait time to see a physician was reported. The trend in mean wait times was minimally affected by the wording change; the 2009 mean wait time to see a physician (57.2 minutes) was not statistically different from mean wait time to see a physician, physician assistant, or nurse practitioner (58.1 minutes). The median wait time to see a physician (33 minutes) was also not affected by the wording change in NHAMCS. In this report, wait times were not presented for visits not seen by a physician, physician assistant, or nurse practitioner (4.1%).
Data analyses were performed using the statistical packages SAS version 9.2 (SAS Institute, Cary, N.C.) and SUDAAN version 9.0 RTI International, Research Triangle Park, N.C.). Differences in average wait times for treatment by ED and patient visit characteristics were examined using t tests for differences at the 0.05 level.
About the authors
Esther Hing and Farida Bhuiya are with the Centers for Disease Control and Prevention's National Center for Health Statistics, Division of Health Care Statistics.
References
- McCaig LF, Burt CW. National Hospital Ambulatory Medical Care Survey: 1999 emergency department summary. Advance data from vital and health statistics; no 320. Hyattsville, MD: National Center for Health Statistics. 2001.
- National Center for Health Statistics. National Hospital Ambulatory Medical Care Survey: 2009 emergency department summary tables.
- Institute of Medicine, Committee on the Future of Emergency Care in the United States Health System. Hospital-based emergency care: At the breaking point. Washington, DC: National Academies Press. 2007.
- U.S. Government Accountability Office. Hospital emergency departments: Crowding continues to occur, and some patients wait longer than recommended time frames. A report to the Chairman, Committee on Finance, U.S. Senate. Washington, DC: Publication No. GAO–09–347 2009.
- McCaig LF, Burt CW. National Hospital Ambulatory Medical Care Survey: 2003 emergency department summary. Advance data from vital and health statistics; no 358. Hyattsville, MD: National Center for Health Statistics. 2005.
- Burt CW, McCaig LF, Valverde RH. Analysis of ambulance diversions in U.S. emergency departments. Ann Emerg Med 47(4):317–26. 2006.
- Wilper AP, Woolhandler S, Lasser KE, McCormick D, Cutrona SL, Bor DH, Himmelstein DU. Waits to see an emergency department physician: U.S. trends and predictors, 1997–2004. Health Aff 27(2):W84–95. 2008.
- American College of Emergency Physicians Crowding Resources Task Force. Responding to emergency department crowding: A guidebook for chapters. Dallas, TX. 2002.
- National Center for Health Statistics. NHAMCS Micro-data File Documentation. 2009. [PDF - 1.4 MB].
Suggested citation
Hing E, Bhuiya F. Wait time for treatment in hospital emergency departments: 2009. NCHS data brief, no 102. Hyattsville, MD: National Center for Health Statistics. 2012.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Edward J. Sondik, Ph.D., Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Division of Health Care Statistics
Clarice Brown, M.S., Director
- Page last reviewed: November 6, 2015
- Page last updated: August 28, 2012
- Content source: