

Slide Set G: Program Integration: The New York Experience
 ShareCompartir
ShareCompartir
This website is archived for historical purposes and is no longer being maintained or updated.
Download the complete slide set:
- 20 Slides in Adobe PDF Format - [970KB]
- 20 Slides in PowerPoint PPT Format - [1MB]
- 20 Slides in Adobe Flash Format - [363KB]

While the content is in the public domain and no copyright restriction applies, we do ask that users preserve the slides in their current format and cite CDC as the source.
Slide 1
Integration of HIV/AIDS, STD, TB and Viral Hepatitis New York State's Experience
PDF File or PPT File

Slide 2
Why Integration?
PDF File or PPT File
Slide 3
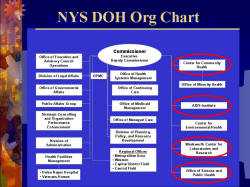
NYS DOH Org Chart
PDF File or PPT File
Slide 4
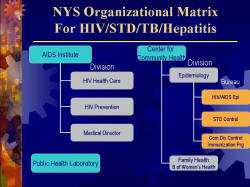
NYS Organizational Matrix
PDF File or PPT File

Slide 5
Important Related Offices for Integration
PDF File or PPT File
Slide 6
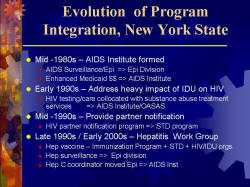
Evolution of Program Integration, New York State
PDF File or PPT File

Slide 7
Multiple Approaches to Program Integration
PDF File or PPT File

Slide 8
Avoid Over-Reorganization
PDF File or PPT File

Slide 9
NYS Approach to Integration
PDF File or PPT File

Slide 10
Integration Example: Hepatitis
PDF File or PPT File
Slide 11
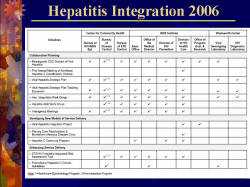
Hepatitis Integration 2006
PDF File or PPT File

Slide 12
Hepatitis Integration Successes
PDF File or PPT File
Slide 13
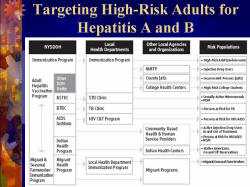
Targeting High-Risk Adults for Hepatitis A and B
PDF File or PPT File
Slide 14
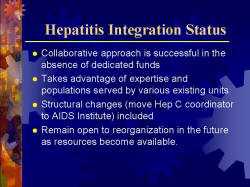
Hepatitis Integration Status
PDF File or PPT File

Slide 15
Impediments to Integration
PDF File or PPT File

Slide 16
Facilitators of Integration
PDF File or PPT File
Slide 17
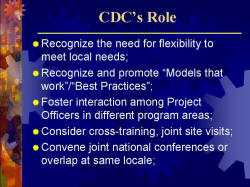
CDC's Role
PDF File or PPT File
Slide 18
CDC's Role
PDF File or PPT File
Slide 19
Summary
PDF File or PPT File

- Page last reviewed: March 5, 2014 (archived document)
- Content source: