

Ciprofloxacin- and Azithromycin-Nonsusceptible Shigellosis in the United States
 ShareCompartir
ShareCompartir

This is an official
CDC HEALTH ADVISORY
Distributed via the CDC Health Alert Network
June 4, 2015, 14:00 ET (2:00 PM ET)
CDCHAN-00379
Summary
CDC continues to receive new reports of infections with Shigella strains that are not susceptible to ciprofloxacin and/or azithromycin, the antimicrobial agents most commonly used to treat shigellosis. Most cases have been reported among gay, bisexual, and other men who have sex with men (collectively referred to as MSM) in Illinois, Minnesota, and Montana and among international travelers, but cases are also occurring among other populations. Shigellosis is very contagious and can spread quickly through communities and across different segments of the population.
CDC recommends meticulous handwashing and other hygiene practices to prevent shigellosis and encourages patients with symptoms of shigellosis such as diarrhea and fever to visit a healthcare provider. Clinicians should obtain stool cultures from patients suspected of having shigellosis, counsel patients about shigellosis prevention, and, when treatment is required, select drugs based on antimicrobial susceptibility test results.
This Health Alert Network (HAN) Advisory provides the following:
- Information about the current status of the outbreaks;
- Recommendations for clinical management, counseling, and follow-up of exposed patients and their contacts;
- Recommendations on general prevention methods for the public, childcare centers, MSM, and international travelers;
- Information about testing and interpretation of azithromycin susceptibility among shigellae; and
- Information about revisions to CDC's Shigella website on shigellosis prevention among MSM.
Background
Recent Outbreaks of Multidrug-Resistant Shigella sonnei Infections
- Extremely drug-resistant (XDR) shigellosis: As of May 7, 2015, five confirmed cases of XDR shigellosis were identified with onset dates from September 7, 2014 through April 4, 2015, in Illinois and Montana residents. The isolates were tested by CDC’s National Antimicrobial Resistance Monitoring System (NARMS) and were resistant to ampicillin, ciprofloxacin, nalidixic acid, streptomycin, sulfisoxazole, tetracycline, and trimethoprim/sulphamethoxazole; had azithromycin minimum inhibitory concentrations >16 µg/ml; and harbored macrolide resistance genes mphA and ermB. Of the five cases, three self-identified as MSM and two are known to have experienced >14 days of diarrhea. Additionally, in March 2015, a Colorado resident who self-identified as MSM was infected with S. sonnei that was resistant to ciprofloxacin, nalidixic acid, and trimethoprim/sulphamethoxazole, and had azithromycin minimum inhibitory concentrations >16 µg/ml. All six of these cases yielded a pulsed-field gel electrophoresis (PFGE) pattern indistinguishable from those associated with an ongoing cluster summarized in 2) below.
- Ciprofloxacin-resistant shigellosis: From May 2014 through April 2015, 179 cases with one of five highly-related PFGE patterns were identified in 34 states and Puerto Rico; approximately half of those who provided information reported international travel before illness onset. Ten of the cases identified by PulseNet, and another 115 cases without PFGE data, were part of an outbreak in San Francisco, California. All San Francisco isolates, and 89% of isolates overall, were resistant to ciprofloxacin. Nineteen cases are known to have occurred among MSM, and several MSM sub-clusters have been reported throughout the United States. A sub-outbreak in a childcare center made 16 people ill. Please see the MMWR report for more information: (http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6412a2.htm?s_cid=mm6412a2_e).
- Shigellosis with decreased susceptibility to azithromycin (DSA):[1] MSM in Chicago, Illinois, and metropolitan Minneapolis/St. Paul, Minnesota, were involved in an outbreak from May 13 through December 8, 2014. Twenty-two isolates displayed highly similar PFGE patterns and had DSA; two additional isolates had indistinguishable PFGE patterns but did not undergo antimicrobial susceptibility testing. All 22 patients were adult males; 15 of 17 with information self-identified as MSM, and 12 were known to have HIV infection. An additional case with an indistinguishable PFGE pattern occurred in an MSM in San Francisco in January 2015, but the isolate was not available for azithromycin susceptibility testing. Please see the MMWR report for more information: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6421a7.htm?s_cid=mm6421a7_w
Figure 1
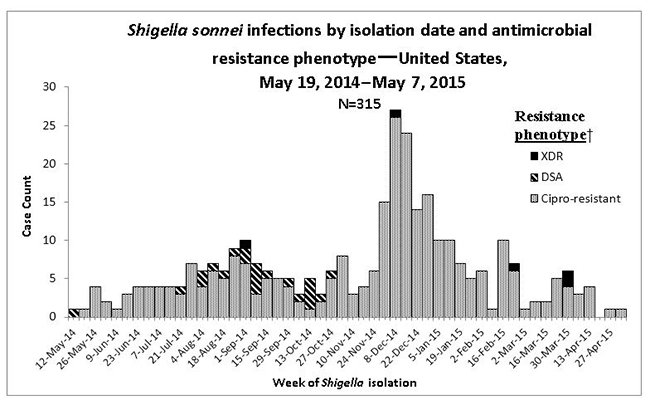
†DSA, decreased susceptibility to azithromycin. XDR, resistant to at least ampicillin, trimethoprim/sulfamethoxazole, and ciprofloxacin, and with decreased susceptibility to azithromycin
General Prevention Recommendations
- Always practice good hygiene, such as washing hands with soap before preparing food or eating and after using the toilet, and follow the recommendations below.
- Childcare centers should:
- Ensure handwashing stations are at the appropriate height for young children, well-stocked with soap and paper towels, and located near diapering, toilet, food preparation, and dining areas.
- Require handwashing among children and staff upon arrival at the facility, after diaper changes and toileting, after outdoor play, before eating, and before departing the facility.
- Follow proper diapering procedures. For more information about this, see: http://www.cdc.gov/healthywater/pdf/hygiene/Diapering-procedures-childcare-508c.PDF
- Assign separate staff to food preparation and diapering.
- Avoid providing wading pools or basins of water for sensory play.
- Exclude children and staff with diarrhea as directed by local ordinances.
- MSM should:
- Avoid sex while ill or while partners are ill with diarrhea and for a few weeks after recovering.
- Wash hands, genitals, and anus with soap before and after sex.
- Use barriers such as dental dams and gloves during anal rimming and fisting.
- Use condoms during anal or oral sex.
- For more information about Shigella infections among MSM, see http://www.cdc.gov/shigella/msm.html.
- International travelers should:
- Strictly observe food, water, and hand hygiene precautions. For more information about this, see http://wwwnc.cdc.gov/travel/page/food-water-safety.
- Consider taking bismuth subsalicylate (e.g., Pepto-Bismol, Kaopectate) to prevent travelers’ diarrhea.
Recommendations for Shigellosis Patients
Patients infected with Shigella can protect others through the following actions:
- All patients should:
- Wash hands with soap after using the toilet.
- Not prepare food for others while experiencing diarrhea, if possible.
- Professional food service workers should follow the guidance of their local health department about exclusion from and return to work.
- Not swim for 1 week after recovering from diarrhea.
- Children in childcare and childcare staff should:
- Stay home while ill with shigellosis.
- Follow the guidance of the local health department about return to the childcare facility.
- MSM should:
- Avoid sex while ill with diarrhea and for a few weeks after recovering. Shigellae have been documented in stool for as long as 11 weeks after diarrhea has stopped, although most patients are likely to have shigellae in stool for a shorter period of time. Avoid sex for a few weeks after recovering or until a convalescent stool culture is negative to reduce the likelihood of transmission to sexual partners.
- After resuming sex, protect others by:
- Washing hands, genitals, and anus with soap before and after sex.
- Using barriers such as dental dams and gloves during anal rimming and fisting.
- Using condoms during anal and oral sex.
- For more information about Shigella infections among gay and bisexual men, see http://www.cdc.gov/shigella/msm.html.
Recommendations for Clinicians
- Obtain stool cultures from patients suspected of having shigellosis.
- Base treatment for shigellosis, when needed, on the antimicrobial susceptibility profile of the individual isolate, or during a local outbreak, that of the outbreak strain.
- Counsel shigellosis patients about the importance of meticulous handwashing after using the toilet, and avoiding activities most likely to transmit the infection to others, such as preparing food for others, swimming, group play among young children, and certain sexual activities (e.g., anal rimming or fisting).
- Recommend symptomatic contacts of shigellosis patients, particularly those suspected to have a multidrug-resistant strain, seek health care.
- For shigellosis patients with treatment failure or prolonged diarrhea, obtain follow-up stool cultures at short intervals (e.g., semi-weekly) until the patient has a negative culture. Shedding of multidrug-resistant shigellae in feces may be prolonged, particularly if the patient was treated with an antimicrobial medication to which the isolate was resistant. Confirming clearance of shigellae from stool will allow more accurate counseling about the timelines appropriate for return to higher-risk activities.
Testing and Interpretation of Azithromycin Susceptibility among Shigellae
Antimicrobial susceptibility testing guidelines and interpretive criteria for azithromycin and Shigella have not been published by clinical laboratory organizations, such as the Clinical and Laboratory Standards Institute. CDC’s National Antimicrobial Resistance Monitoring System (NARMS) has developed a protocol to test Shigella for susceptibility to azithromycin using the disk diffusion method. Health department and clinical laboratories that wish to use the protocol for epidemiologic purposes may contact Davina Campbell at xew9@cdc.gov for more information.
Revisions to CDC's Shigella Website, Including Prevention among MSM
CDC recently updated the Frequently Asked Questions page on its Shigella website (http://www.cdc.gov/shigella/general-information.html). In addition, CDC developed new guidance and a fact sheet on prevention of shigellosis among MSM (http://www.cdc.gov/shigella/msm.html).
For More Information
- For more information on Shigella, see http://www.cdc.gov/shigella/index.html or contact Jacqueline Hurd at xyf2@cdc.gov.
The Centers for Disease Control and Prevention (CDC) protects people's health and safety by preventing and controlling diseases and injuries; enhances health decisions by providing credible information on critical health issues; and promotes healthy living through strong partnerships with local, national and international organizations.
Department of Health and Human Services
HAN Message Types
- Health Alert: Conveys the highest level of importance; warrants immediate action or attention. Example: HAN00001
- Health Advisory: Provides important information for a specific incident or situation; may not require immediate action. Example: HAN00346
- Health Update: Provides updated information regarding an incident or situation; unlikely to require immediate action. Example: HAN00342
- Info Service: Provides general information that is not necessarily considered to be of an emergent nature. Example: HAN00345
###
This message was distributed to state and local health officers, state and local epidemiologists, state and local laboratory directors, public information officers, HAN coordinators, and clinician organizations.
###
Additional Resources
- Page last reviewed: June 4, 2015
- Page last updated: June 4, 2015
- Content source:
- Division of Emergency Operations (DEO); Office of Public Health Preparedness and Response (OPHPR)
- Maintained By: