Mitrofanoff procedure
The Mitrofanoff procedure also known as the Mitrofanoff appendicovesicostomy, is a surgical procedure in which the appendix is used to create a conduit between the skin surface and the urinary bladder. It was named after its developer, Paul Mitrofanoff.[2]
| Mitrofanoff procedure | |
|---|---|
 | |
| Other names | Mitrofanoff appendicovesicostomy |
Description of procedure
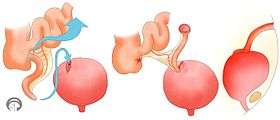
In the procedure, the surgeon separates the appendix from its attachment to the cecum, while maintaining its blood supply, then creates an opening at its blind end and washes it. One end is connected by surgical sutures to the urinary bladder, and the other is connected to the skin to form a stoma. Generally, an incision is made into the navel so it may serve as the canal for the catheter.
Urine is typically drained several times a day by use of a catheter inserted into the Mitrofanoff canal.
Indications
The procedure is typically performed when the normal outlet is blocked (as in urethral cancer) or when frequent, often uncomfortable, catheterizations are needed (as in neurogenic bladder).
Most patients who undergo this procedure are those who are dependent on catheterization to eliminate urine, such as paraplegic individuals or those born with spina bifida. The Mitrofanoff procedure allows the individual to self-catheterize, so assistance from a family member or a medical professional is not needed.
The Mitrofanoff procedure has been found to improve the lives of people with spinal cord injuries, by increasing their independence.[3]
Relation to MACE
The Malone antegrade continence enema (MACE), used to treat fecal incontinence, is like the Mitrofanoff procedure as it uses the Mitrofanoff principle and, thus, can be considered an analogous procedure.
As fecal and urinary incontinence frequently co-exist, a MACE is often created at the same time as a continent catheterizable urinary conduit.[4]
Relation to Monti procedure
If the appendix is not available, due to appendectomy, or unusable for another reason, the Monti procedure is done.[5]
References
- Breen, Micheál; Phelps, Andrew; Estrada, Carlos; Chow, Jeanne S. (2015-09-01). "The role of imaging in pediatric bladder augmentation". Pediatric Radiology. 45 (10): 1440–1447. doi:10.1007/s00247-015-3349-1. ISSN 1432-1998. PMID 25903841.
- Mingin GC, Baskin LS (2003). "Surgical management of the neurogenic bladder and bowel". Int Braz J Urol. 29 (1): 53–61. doi:10.1590/S1677-55382003000100012. PMID 15745470.
- Merenda LA, Duffy T, Betz RR, Mulcahey MJ, Dean G, Pontari M (2007). "Outcomes of Urinary Diversion in Children With Spinal Cord Injuries". J Spinal Cord Med. 30 Suppl 1 (Suppl 1): S41–7. doi:10.1080/10790268.2007.11753968. PMC 2031994. PMID 17874686.
- Teichman JM, Rogenes VJ, Barber DB (1997). "The utility of the Malone antegrade continence enema for urologists". Tech Urol. 3 (1): 30–3. PMID 9170222.
- Shapiro E (1999). "Early Clinical Experience With Monti Procedure and Managing the Nonpalpable Testis in Children". Rev Urol. 1 (2): 94–6. PMC 1476142. PMID 16985779.