Biliary ultrasound
Contents
Background
- Bedside ultrasound can be effectively used to assess for acute cholecystitis
- ED providers have a Sp 96% and Sn 88% using bedside ultrasound[1]
Indications
- RUQ pain
Technique
- Select probe
- Curvilinear/large convex probe
- Phased array probe used by many providers as well
- Location
- Scan from midline to the midclavicular line at the right 11th/12th intercostal spaces
- Move the probe superior or inferior as needed to achieve adequate views
- Alternatively start in RUQ FAST view and scan through inferior aspect of liver, which allows better use of liver as viewing window
- Landmarks
- Exclamation Point Sign: Portal vein and main lobar fissure (MLF)
- Obtain sagittal and transverse images
- Optimize image quality
- Patient in Left lateral decubitus (if can tolerate)
- Allows for better visualization of gallbladder and gallstones
- Stones might shift, polyps or stones impacted in the GB neck will not
- Patient in Left lateral decubitus (if can tolerate)

Findings
Evaluate gallbladder for:
- Gallstones
- identify by hypoechoic "shadowing" behind hyperechoic stones
- if no shadowing, may be polyps, sludge, etc.
- SIN Sign: Stone in neck
- Gallbladder wall thickness
- Pericholecystic free fluid
- Common Bile Duct (CBD) measurement
- Measure from inner to inner
- Sonographic Murphy's sign
- Pain with ultrasound probe palpation over gallbladder
Normal Findings
- No gallstones
- Gallbladder anterior wall <4 mm
- No pericholecystic free fluid
- Common bile duct < 4 mm plus 1mm per decade after 40 yrs old
- Absent sonographic Murphy's sign
Images
Normal

Abnormal

Gallbladder wall thickening

Acute cholecystitis
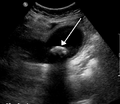
Actue cholecystitis: Gallstone impacted in the neck of the gallbladder with gallbladder wall thickening

Pearls and Pitfalls
- Easily confused with duodenum (hint - look for peristalsis)
- Only measure the anterior wall as the posterior can be enlarged secondary to artifact
- Gallbladder wall thickening can be caused by:
- Acute cholecystitis
- Ascites
- CHF
- Contracted GB: Three distinct wall layers is not pathological
- GB Polyp: Soft tissue masses attached to the wall of the gallbladder and differentiated from gallstones by their lack of mobility and shadowing
- Renal Cyst: Cysts in the superior pole of the kidney (hint - get two views)
- Ascitic fluid: Located throughout peritoneum, including Morison’s pouch though pericholecystic fluid is localized to the anterior side of the gallbladder
Documentation
Normal Exam
A bedside ultrasound was conducted to assess for signs of cholecystitis with clinical indications of RUQ pain. The gallbladder was identified and viewed in the transverse and sagittal plane. There were no gallstones, gallbladder wall thickening, pericholecystic fluid, or sonographic Murphy’s sign. There was no sonographic evidence of acute cholecystitis.
Abnormal Exam
A bedside ultrasound was conducted to assess for signs of cholecystitis with clinical indications of RUQ pain. The gallbladder was identified and viewed in the transverse and sagittal plane. There were gallstones, gallbladder wall thickening of 8mm, pericholecystic fluid, and positive sonographic Murphy’s sign. There are indications of acute cholecystitis.
Clips
Normal Gallbladder
Normal Gallbladder in Sagittal Plane

Normal Gallbladder in Transverse Plane

Abnormal Gallbladder
Edematous Gallbladder

Gallstones

Pitfalls
Contracted Gallbladder

Misidentification of the Duodenum

External Links
See Also
References
- ↑ Kendall JL, Shimp RJ. Performance and interpretation of focused right upper quadrant ultrasound by emergency physicians. J Emerg. Med. 2001; 21(1):7-13.