We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Traumatic pneumothorax
From WikEM
(Redirected from Traumatic Pneumothorax)
Contents
Background
- Present in 25% of patients with chest trauma
Types
- Open
- Communication between pleural space and atmospheric pressure (sucking chest wound)
- Closed
- Occult
- Positive pressure ventilation (e.g. intubation) can convert an occult pneumothorax to a tension pneumothorax
Clinical Features
- Rib fracture and penetrating trauma most common causes
- Isolated pneumothorax does not cause severe symptoms until >40% of hemithorax is occupied
Differential Diagnosis
Pneumothorax Types
- Tension pneumothorax
- Spontaneous pneumothorax
- Traumatic pneumothorax
Thoracic Trauma
- Airway/Pulmonary
- Cardiac/Vascular
- Musculoskeletal
- Other
Evaluation
- Occult pneumothorax after a stab wound may be delayed for up to 6 hours
- If patient decompensates, obtain repeat imaging
Clinically Stable
Defined as having all of the following:
- Resp rate < 24
- Heart rate 60-120 beats per minute
- Normal BP
- SaO2 >90% on room air and patient can speak in whole sentences
Workup

- CXR
- Displaced visceral pleural line without lung markings between pleural line and chest wall
- Upright is best
- Expiratory films DO NOT improve accuracy[1]
- Supine CXR = deep sulcus sign
- CT Chest
- Very sensitive and specific
- Ultrasound
- NO comet tail artifact
- No sliding lung sign
- Bar Code appearance on M-mode (absence of "seashore" waves)
Estimating Pneumothorax Size
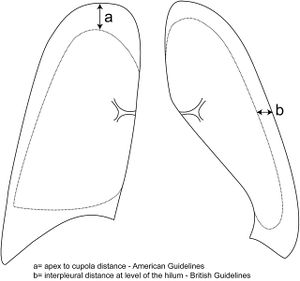
- On a conventional, upright posterior-anterior chest radiograph:
- Very small: <1 cm interpleural distance (confined to upper 1/3 of chest) OR only seen on CT
- Small: ≤3cm lung apex to cupola (chest wall apex) on CXR
- Large: >3cm lung apex to cupola (chest wall apex) on CXR
- 3cm apex to cupola measurement is roughly equivalent to 2cm interpleural distance (at the level of the hilum)
- Both roughly correlate with a 50% pneumothorax by volume
Management
Supplemental oxygen with non-rebreather for all
Tension pneumothorax
- Immediate needle thoracostomy followed by chest tube
Open pneumothorax
- Cover wound with three-sided dressing
- Make sure to avoid complete occlusion (may convert injury to a tension pneumothorax)
Closed traumatic pneumothorax
- Tube thoracostomy indicated if:
- Cannot be observed closely
- Requires intubation
- Will be transported by air or over a long distance
- Observation if:
- Very small AND does not require mechanical ventilation
- Unchanged on repeat CXR in 6 hours
- Decision to intubate
- Intubation can lead to positive pressure which may worsen a stable traumatic pneumothorax
- If patient stable, perferrable to just perform thoracostomy
- If GCS < 8 or patient having difficulty, they should be intubated
Adult Chest Tube Sizes
| Chest Tube Size | Type of Patient | Underlying Causes |
| Small (8-14 Fr) |
|
|
| Medium (20-28 Fr) |
|
|
| Large (36-40 Fr) |
|
|
Disposition
Admit
Special Instructions
Flying
- Can consider flying 2 weeks after full resolution of traumatic pneumothroax[2]
See Also
References
- ↑ Eur Respir J. 1996 Mar;9(3):406-9
- ↑ "Management of spontaneous pneumothorax: British Thoracic Society pleural disease guideline 2010" British Thoracic Society Guidelines. Thorax 2010;65:ii18-ii31 doi:10.1136/thx.2010.136986 PDF