We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Salter-Harris fractures
From WikEM
(Redirected from Salter-Harris fracture)
Contents
Background
- The higher the classification, the higher the likelihood of growth abnormalities
- If physis fracture missed may lead to premature closure and bone growth arrest
- It was previously taught that ligaments are stronger than bones in kids (and fractures were more likely than sprains), however newer studies (to date in ankles) contradict that assumption[1]
Mnemonic
- S 1 - Slipped (thru epiphysis)
- A 2 - Above (epiphysis with metaphysis fracture)
- L 3 - Lower (thru epiphysis)
- T 4 - Through (epinephrine and meta)
- R 5 - Rammed (growth plate crushed)
Fracture Chart
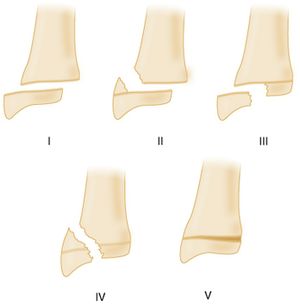
| Type | I (Slip) | II (Above) | III (Below) | IV (Through) | V (Crush) |
| Fracture Location | hypertrophic zone of physis (epiphysis separates from metaphysis) | Through physis and out through piece of metaphyseal bone | Intra-articular | Starts at articular surface and extends through epiphysis, physis, metaphysics | Physis compression |
| Pathophysiology | Growing cells remain on the epiphysis in continuity with blood supply | Growing cells remain on the epiphysis in continuity with blood supply | fracture extends from epiphysis through physis | ||
| Epidemiology | Occurs mostly in infants and todlers | Most common type of fracture | Typically occurs at knee or ankle | ||
| Prognosis | Good | Good | Moderate | Moderate | Highest chance of growth arrest |
Clinical Features
- Trauma with point tenderness over a non-closed (pediatric) physis
Differential Diagnosis
- Sprain
- Contusion
- Other fracture
Evaluation
Type 1 (Slip)
- Suspect if point tenderness over a physis
- X-ray findings are subtle (epiphyseal displacement) or absent (clinical diagnosis)
Type 2 (Above)
- X-ray shows triangular fragment of metaphysis with out injury to epiphysis
Type 3 (Below)
- X-ray shows epiphyseal fragment not associated with etaphyseal fracture
- Greater the displacement greater chance of vascular supply compromise
Type 4 (Both)
- fracture starts at articular surface and extends through epiphysis, physis, metaphysics
Type 5 (Crush)

- X-ray shows physis compression fracture
- May confuse for Type 1 injury
- X-ray findings may be minimal
Management
Type I
- Most: Splint, ortho follow up
- Lateral ankle:
- Removable ankle brace
- Return to activities as tolerated by pain
- No ortho followup
Type II
- Most: Splint, ortho follow up
- Ankle: Removable ankle brace[2]
Type III-V
- Splint, ortho consult
Disposition
- Outpatient
See Also
External Links
- POSNA (Pediatric Orthopaedic Society of North America) - http://orthoinfo.aaos.org/topic.cfm?topic=A00040
References
- ↑ Blackburn EW, Aronsson DD, Rubright JH, Lisle JW. Ankle fractures in children. J Bone Joint Surg Am. 2012; 94(13):1234-1244.
- ↑ . Boutis K, Willan AR, Babyn P, Narayanan UG, Alman B, Schuh S. A randomized, controlled trial of a removable brace versus casting in children with low-risk ankle fractures. Pediatrics. 2007;119(6): e1256-e1263.