We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Intraosseous access
From WikEM
(Redirected from IO access)
Contents
Indications
- Immediate vascular access required for administration of drugs/fluids
- Cardiac arrest, resuscitation when no other IV in place

Contraindications
- Osteoporosis
- Osteomyelitis
- Osteogenesis imperfecta
- Fractured bone
- Recent IO infusion in same bone
- Cellulitis, Infection, or Burn, at insertion site
Equipment
- EZ-IO drill (other products/brands available)
- Appropriate IO needle with extension set
- Chloraprep or alcohol swabs
- Saline Flush
- Lidocaine (2% lidocaine without epi)
Site Selection
- Proximal Tibia- 2 finger breadths below tibial tuberosity (1-3 cm) on medial, flat aspect of tibia
- Distal Tibia- medial surface at junction of medial malleolus and shaft of tibia, posterior to to greater saphenous vein
- Proximal humerus (adults only, use yellow needle) [1]
- keep arm adducted and internally rotated (hand on bellybutton)
- slide fingers up humerus until you feel a notch (surgical neck)
- insert IO 1cm above surgical neck into the greater tubercle
- immobilize arm or IO will displace (no abduction at shoulder)
- Distal Femur (generally only in infants and children)
- Pelvic ASIS
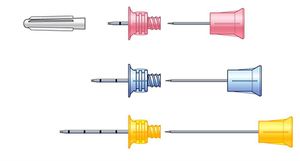
EZ-IO Needle selection (based on weight of patient)
- Pink 15mm (3-39kg)
- Blue 25mm (40kg and above)
- Yellow 45mm (excessive tissue)
Procedure
- Identify landmarks
- Clean skin
- Place appropriate needle on drill and remove safety cap
- ADVANCE needle through skin to bone
- DRILL needle perpendicular into bone at site with gentle, constant pressure
- When needle tip contacts bone there should be 5mm of catheter visible outside of skin (if not you may need a longer needle)
- Continue drilling through bone until "give" or "pop" occurs and needle tip enters medullary space
- Remove stylet (caution: stylet is extremely sharp - place in sharps container)
- Attach the manuacturer's extension set (helpful if this is pre-flushed with saline and/or lidocaine)
- Aspirate blood/marrow to confirm placement
- If patient is awake, slowly infuse 2% lidocaine (cardiac lidocaine) 2-3mL through the IO line (IO infusion is painful as the marrow cavity expands)
- Flush saline through extension set to expand marrow cavity (helps ensure adequate flow rates)
- Apply dressing
Removal
- Detach extension tubing. Gently and slowly apply in-line traction (i.e. pull straight out - do not rock back and forth). May rotate clockwise while applying in-line traction.
- Can attach syringe via luer lock to act as handle
- Apply dressing.
(IO's should not be left in more than 72-96 h and ideally removed after initial resuscitation once more secured access is achieved[2])
Complications
- Compartment syndrome
- Incomplete penetration of cortex
- Penetration of posterior cortex
- Infection (cellulitis, osteomyelitis)
- Fracture
- Growth plate damage
- Fat embolism
Labs drawn via IO
- Blood drawn from an IO can be used for type and cross, chemistry, blood gas.
- There is not good correlation with Sodium, Potassium, CO2, and calcium levels.[3]
- Potassium is often elevated due to hemolysis
- CANNOT use IO blood for CBC
- WBCs are higher and platelet counts are lower[3]
IO Medications
- Any medication that can be given in peripheral IV can be given through IO
- Epinephrine infused via the intraosseous humeral site has the identical peak serum concentration as if it were instilled via a subclavian central line[4]
- RSI medications can be given through IO with the same efficacy[5]
- Same doses as IV meds
- Follow with flush
- Drips or IV fluids should be given with pressure bag or infusion pump
IO and CT contrast
- Overall safe and effective
- Case reports with successful venous opacification in a trauma patient [6]
- Successful CTA PE protocol reported [7]
- Connect power injector straight to IO needle. Do not use IO extension tubing (cannot withstand pressure) [8]
See Also
References
- ↑ http://www.acep.org/WorkArea/DownloadAsset.aspx?id=48943
- ↑ Dev SP, et al. Insertion of an intraosseous needle in adults. N Engl J Med. 2014; 370:e35.
- ↑ 3.0 3.1 Miller LJ. et al A new study of intraosseous blood for laboratory analysis.Arch Pathol Lab Med. 2010 Sep;134(9):1253-60.
- ↑ Kramer GC, Hoskins SL, Espana J, et al. Intraosseous drug delivery during cardiopulmonary resuscitation: relative dose delivery via the sternal and tibial routes. Acad Emerg Med 2005;12(5):s67.
- ↑ Barnard, et al. Rapid sequence induction of anaesthesia via the intraosseous route: a prospective observational study. Emerg Med J. 2014; Jun 24. pii: emermed-2014-203740. [Epub ahead of print]
- ↑ Knuth, et al. Intraosseous Injection of Iodinated Computed Tomography Contrast Agent in an Adult Blunt Trauma Patient. Annals of Emergency Medicine. 2011; 57 (4) 382-386
- ↑ Ahrens, et al. Successful Computed Tomography Angiogram Through Tibial Intraosseous Access: A Case Report. Journal of Emergency Medicine. 2013; 45 (2): 182-184
- ↑ Miller, et al. Utility of an intraosseous vascular system to deliver contrast dye using a power injector for computerized tomography studies. Annals of Emergency Medicine. 2011; 58 (4) 240-241.