We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Hand and finger tendon injuries
From WikEM
(Redirected from Hand (Tendon Injuries))
Contents
Background
Tendons of the upper extremity anatomy
- Fingers
- FDP (DIP flexion)
- FDS (PIP flexion)
- Extensor dig communis (extension)
- Mallet = DIP
- Boutonniere = PIP
- Thumb
- Flx pollicis longus (flexion)
- Ex poll longus (DIP ext)
- Ex poll brevis (MCP ext)
- Abductor poll longus (abduction)
- Wrist
- Flexor carpi ulnaris (flx + ulnar deviation)
- Flexor carpi radialis (flx + radial dev)
- Extensor carpi ulnaris (ext + ulnar dev)
- Extensor carpi radialis (ext + radial dev)
Flexor

Management
- Primary repair should occur within 12hr; secondary repair can occur up to 4wk after injury
- Hand surgeon should repair all flexor tendon lacerations
- If hand surgeon is not immediately available:
- Irrigate open wounds and close with 5-0 nylon
- Most advocate antibiotics
- Splint hand with:
- Wrist in 30 deg of flexion
- MCP joints in 70 deg of flexion
- IP joint flexed 10-15 deg of flexion
Extensor
Background
- Most common site of tendon injuries b/c of superfical location on dorsum of hand
- If tendon lac suspected but unable to be located it is ok to refer to specialist within 3d
- Delayed repair up to 7-10d usually has equal outcome to immediate repair
- Zones V-VII Splinting (after repair)
- Requires splinting with:
- Wrist in 15 deg extension
- MCP joint in 15 deg flexion
- IP join in 15 deg flexion in involved and adjacent digit
- Requires splinting with:
Zones
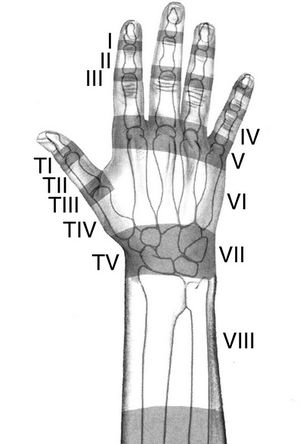
- Zone I
- Area over distal phalanx and DIP joint
- Complete laceration at this level will result in DIP joint flexed 40 degrees
- "Mallet finger" refers to closed disruption of distal extensor apparatus
- Occurs due to sudden forceful flexion of extended finger (finger gets "jammed")
- May occur due to tear of tendon itself or avultion fracture of dorsal base of phalanx
- Most common tendon injury in athletes
- Immobilize DIP joint only in continuous slight hyperextension for 6-8wks
- Zone II
- Area over middle phalanx
- Treatment is similar to zone I injuries
- Zone III
- Area over the PIP joint
- Central tendon is most commonly injured structure
- Controversial whether conservative or operative management is best
- Closed injuries are initially treated with PIP joint immobilized in extension for 5-6wks
- Must be followed closely by hand specialist
- Zone IV
- Involves area over proximal phalanx
- Clinical findings are similar to zone III injuries
- Zone V
- Area over MCP joint
- Open injuries to this area should be considered human bites until proven otherwise
- If it is human bite performed delayed repair following course of antibiotic
- Zone VI
- Area over dorsum of hand
- Tendons in this area are superficial; even minor-appearing lacs are associated with tendon injuries
- Treatment typically requires operative fixation with K wires
- Zone VII
- Area over the wrist
- Repair can be difficult because of presence of extensor retinaculum
- Zone VIII
- Area of the distal forearm
- Tendons frequently retract into the forearm and must be retrieved and repaired
- Lac <25%: does not require repair
- Lac 25-50% requires simple suture repair
- Lac >50% requires specialized repair