We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Formal echocardiography
From WikEM
(Redirected from Diastolic dysfunction)
Diagnostic Pearls
- Normal directional flow in CW and PW in apical, parasternal short:
- Below the line for pulmonic and aortic valves (systole)
- Above the line in tricuspid and mitral valves (diastole)
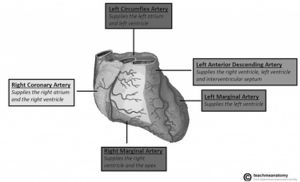
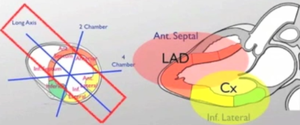
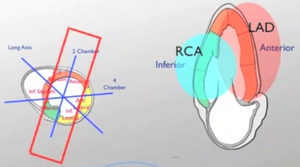
- Coronary artery distributions
- LAD, circumflex, RCA
- Left marginal = obtuse marginal
- Right marginal

Parasternal long
- Assess for mitral valve prolapse, systolic anterior motion
- Differentiate pleural effusion from pericardial effusion
- Pericardial effusion is anterior to descending aorta
- Pleural effusion posterior to descending aorta
Pericardial effusion vs. pleural effusion
- Wall motion assessment obtains LAD and Circumflex coronary artery distributions
- EPSS, E-Point Septal Separation in PSL view
- M-mode distance in mm between anterior leaflet of MV and septum in diastole
- E-point is shortest distance
- LVEF = 75.5 - 2.5 x EPSS in mm[1]
- EPSS and MRI LVEF correlated ~0.80 in study that generated equation
- Excluded MV prostheses, asymmetrical septal hypertrophy, significant aortic regurgitation
- Values as calculated by above study
- < 5 mm, normal
- > 7 mm, EF < 50%
- > 18 mm, EF < 30%
- Falsely elevated EPSS in:
- Mitral stenosis, rheumatic heart disease
- Mitral calcification
- Aortic regurgitation
- LV dilation
Parasternal short
- See Aortic stenosis regarding evaluation of cuspidity
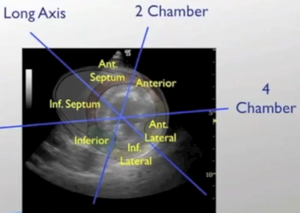
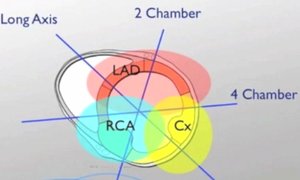
- Evaluate kinetics of LV motion anatomically by coronary artery flow
Apical
- Best obtained in left lateral decubitus with left arm above head to open up ribs
- EF estimation
- LVEF by Simpson, LV volume change
- LVEF by Teichholz method, using M-mode (estimation of LV volume by diameter measured just beyond mitral tips in diastole)
- EF visual assessment:
- >65% = hyperdynamic
- 55-65% = normal
- 45-54% = mildly depressed
- 30-44% = moderately depressed
- <30% = severely depressed
- Evaluation for wall motion abnormality
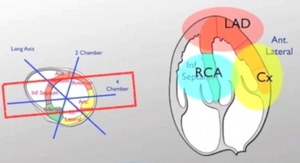
Apical Two Chamber View
- Infrequently used unless concern exists for full evaluation of wall motion abnormality in LV
- Obtains better views of RCA and LAD distribution
Aortic Stenosis
- See Aortic stenosis for formal echo evaluation
Mitral Stenosis
- See Mitral stenosis for formal echo evaluation
Diastolic Function[2]
- Worsening diastolic dysfunction corresponds to less fluid responsive hypotension and more volume overload
- Septic/hypotensive patients with baseline diastolic dysfunction will not have reliable IVC ultrasounding for fluid responsiveness
- Pts in impaired relaxation states can stand to be volume resuscitated just until impaired relaxation becomes pseudonormal
- Otherwise seen as the E wave ≈ A wave (give fluids until E wave increases up to A wave)
- If still hypotensive at that point, pt volume resuscitated, then start vasopressors
- Patients with pseudonormal or worse diastolic dysfunction require vasopressors, not more fluids
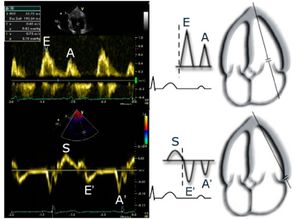
- Measure E and A waves, then e' and a' waves with tissue doppler
- PW Doppler across MV in apical view bisecting across MV tips during opening, diastole
- Tissue doppler at MV annulus (base) at either septum or lateral position to measure tissue velocity
- E/e' ratio ≅ LVEDP (PCWP)
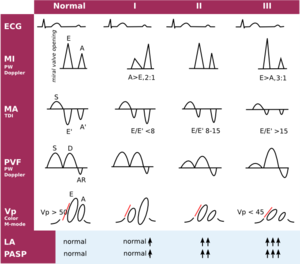
- Rule 1: Normal diastolic function if echo normal, age<45 yrs, E>A
- Rule 2: Impaired relaxation if A>E, with E/A<1
- Rule 3: Pseudonormal if echo abnormal (LVH), age>65, E>A, E/A>1
- Rule 4: Restrictive filling if E/A>2

{kind=link}
- Evaluate the E' and A' in tissue doppler to differentiate normal diastolic function from pseudonormalization[4]
- Septal MV annulus TD, E' magnitude less than 8 cm/s suggestive of diastolic dysfunction
- Lateral MV annulus TD, E' < 10 cm/s suggestive of diastolic dysfunction
| Normal | Impaired | Pseudonormal | Restrictive | |
| LVEDP | < 15 mmHg | < 15 mmHg | 15-25 mmHg | > 25 mmHg |
| E velocity | Normal | Stays Same | ~ 100 cm/s | ~150 cm/s |
| A velocity | Normal | ↑ | ↓ | ↓↓ |
| E/A | > 1 | < 1 | > 1 | > 2 |
| TDI | e' > a' | a' > e' | a' > e' | a' ≈ e' |
| E/e' | < 15 | < 15 | > 15 | > 15 |
| e' (septal) | > 8 cm/s | < 8 cm/s | << 8 cm/s | <<< 8 cm/s |
Two chamber view
Three chamber view
Subxiphoid view
Suprasternal view
See Also
- Aortic stenosis for CW Doppler measurements
- ECHOpedia Diastolic Dysfunction
External Links
References
- ↑ Silverstein JR et al. Quantitative Estimation of Left Ventricular Ejection Fraction from Mitral Valve E-Point to Septal Separation and Comparison to Magnetic Resonance Imaging. Jan 2006. Vol 97, Issue 1, Pg 137=140.
- ↑ Dokainish H. Left ventricular diastolic function and dysfunction: Central role of echocardiography. Glob Cardiol Sci Pract. 2015; 2015: 3.
- ↑ 123sonography. Nov 20, 2010. https://www.youtube.com/watch?v=qdLkbcFe_DI.
- ↑ Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA, Waggoner AD, Flachskampf FA, Pellikka PA, and Evangelisa A. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. Eur J Echocardiogr. 2009 Mar;10(2):165-93.