We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Patella dislocation
From WikEM
Contents
Background
- Occurs with trauma to an extended knee with externally rotated foot and twisting motion[1]
- Acute: in traumatic injury, occurs equally in men/women [2]
- Chronic: women/teenage girls[2]
- Commonly lateral displacement and unable to extend knee
Clinical Features

- Patella is usually displaced laterally; knee is held in flexion
- Acute: often with large hemarthrosis
- Chronic: little to no swelling
Differential Diagnosis
Knee diagnoses
Acute Injury
- Knee fractures
- Patella fracture
- Tibial plateau fracture
- Knee dislocation
- Patella dislocation
- Segond fracture
- Meniscus and ligament knee injuries
- Patellar Tendinitis (Jumper's knee)
- Patellar tendon rupture
- Quadriceps tendon rupture
Nontraumatic/Subacute
- Septic Joint
- Gout
- Popliteal cyst (Baker's)
- Prepatellar bursitis (nonseptic)
- Septic bursitis
- Pes anserine bursitis
- Patellofemoral syndrome (Runner's Knee)
- Patellar Tendinitis (Jumper's knee)
- Osgood-Schlatter disease
- Arthritis
Evaluation
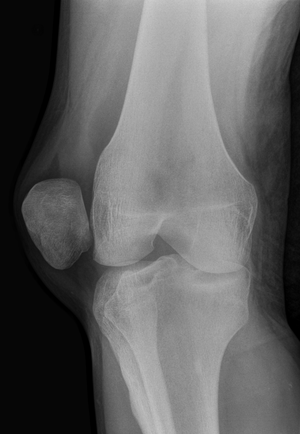
- Xray if traumatic mechanism to rule out fracture
- Do not need xay prior to reduction if chronic
- Post-reduction x-ray: confirm reduction, eval for fractures and loose bodies (avulsions, misalignment, etc)[3]
- Common associated fractures
- Medial patella facet
- Lateral femoral condyle
Management
- Reduce; do not need x-rays prior to reduction. Rarely need any sedation though a dose of IV pain medication can help relax the patient
- Option #1:
- Mild flexion of hip (20-30 degrees by raising head of bed, not by propping the leg up off the bed) to relax quadriceps
- Slowly extend and slightly hyperextend the knee and slide patella back into place.
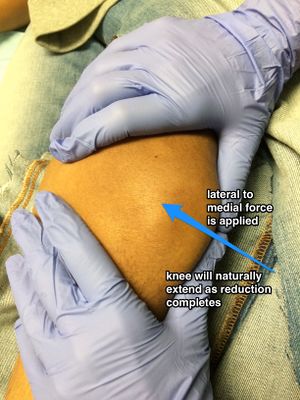
- Option #2
- One provider applies slow downward pressure over the quads. This stretches out the muscle and slowly straigttens the leg
- At the same time, second pulls gentle traction of the patella outward while rotating the patella back over from lateral to anterior
- Knee immobilizer, NSAIDs, weight-bearing as tolerated
- Option #1:
Disposition
- Orthopedic follow-up within 1-2wks
- Unable to reduce or loose bodies/fracture on post-reduction imaging
- Obtain immediate ortho consult
References
- ↑ Review of Orthopaedics, 6th Edition, Mark D. Miller MD, Stephen R. Thompson MBBS MEd FRCSC, Jennifer Hart MPAS PA-C ATC, an imprint of Elsevier, Philadelphia, Copyright 2012
- ↑ 2.0 2.1 Fithian DC, Paxton EW, Stone ML, Silva P, Davis DK, Elias DA, White LM. Epidemiology and natural history of acute patellar dislocation. AJSM 2004;32:1114-1121
- ↑ Krause E A. et al. Pediatric lateral patellar dislocation: is there a role for plain radiography in the emergency department? J Emerg Med. 2013 Jun;44(6):1126-31
See Also
Authors
Aaron Snyder, Jay, Jordan Swartz, Daniel Ostermayer, Michael Holtz, Ross Donaldson, Ted Fan, Neil Young, Claire