Wernicke's area
Wernicke's area (/ˈvɛərnɪkə/ or /ˈvɛərnɪki/; German: [ˈvɛʁnɪkə]), also called Wernicke's speech area, is one of the two parts of the cerebral cortex that are linked to speech (the other is Broca's area). It is involved in the comprehension of written and spoken language (in contrast to Broca's area that is involved in the production of language). It is traditionally thought to be in Brodmann area 22, which is located in the superior temporal lobe in the dominant cerebral hemisphere (which is the left hemisphere in about 95% of right handed individuals and 60% of left handed individuals).
| Wernicke's area | |
|---|---|
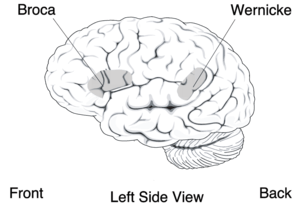 Wernicke's area is located in the temporal lobe, shown here in grey | |
| Details | |
| Location | Temporal lobe of the dominant cerebral hemisphere. |
| Artery | Branches from the middle cerebral artery |
| Identifiers | |
| MeSH | D065813 |
| NeuroNames | 1233 |
| NeuroLex ID | nlx_144087 |
| FMA | 242178 |
| Anatomical terms of neuroanatomy | |
Damage caused to Wernicke's area results in receptive, fluent aphasia. This means that the person with aphasia will be able to fluently connect words, but the phrases will lack meaning. This is unlike non-fluent aphasia, in which the person will use meaningful words, but in a non-fluent, telegraphic manner.[1]
Structure
Wernicke's area is classically located in the posterior section of the superior temporal gyrus (STG) in the (most commonly) left cerebral hemisphere. This area encircles the auditory cortex on the lateral sulcus (the part of the brain where the temporal lobe and parietal lobe meet).[2] This area is neuroanatomically described as the posterior part of Brodmann area 22.
However, there is an absence of consistent definitions as to the location.[3][4] Some identify it with the unimodal auditory association in the superior temporal gyrus anterior to the primary auditory cortex (the anterior part of BA 22).[5] This is the site most consistently implicated in auditory word recognition by functional brain imaging experiments.[6][7] Others include also adjacent parts of the heteromodal cortex in BA 39 and BA40 in the parietal lobe.[8]
While previously thought to connect Wernicke's area and Broca's area, new research demonstrates that the arcuate fasciculus instead connects to posterior receptive areas with premotor/motor areas, and not to Broca's area.[9] Consistent with the word recognition site identified in brain imaging, the uncinate fasciculus connects anterior superior temporal regions with Broca's area.[10]
Function
Right homologous area
Research using Transcranial magnetic stimulation suggests that the area corresponding to the Wernicke’s area in the non-dominant cerebral hemisphere has a role in processing and resolution of subordinate meanings of ambiguous words—such as ‘‘river’’ when given the ambiguous word "bank." In contrast, the Wernicke's area in the dominant hemisphere processes dominant word meanings (‘‘teller’’ given ‘‘bank’’).[11]
Modern views
Neuroimaging suggests the functions earlier attributed to Wernicke's area occur more broadly in the temporal lobe and indeed happen also in Broca's area.
| “ | There are some suggestions that middle and inferior temporal gyri and basal temporal cortex reflect lexical processing ... there is consensus that the STG from rostral to caudal fields and the STS constitute the neural tissue in which many of the critical computations for speech recognition are executed ... aspects of Broca’s area (Brodmann areas 44 and 45) are also regularly implicated in speech processing.
... the range of areas implicated in speech processing go well beyond the classical language areas typically mentioned for speech; the vast majority of textbooks still state that this aspect of perception and language processing occurs in Wernicke’s area (the posterior third of the STG).[12] |
” |
Support for a broad range of speech processing areas was furthered by a recent study caried out at the University of Rochester in which American Sign Language native speakers were subject to MRI while interpreting sentences that identified a relationship using either syntax (relationship is determined by the word order) or inflection (relationship is determined by physical motion of "moving hands through space or signing on one side of the body"). Distinct areas of the brain were activated with the frontal cortex (associated with ability to put information into sequences) being more active in the syntax condition and the temporal lobes (associated with dividing information into its constituent parts) being more active in the inflection condition. However, these areas are not mutually exclusive and show a large amount of overlap. These findings imply that while speech processing is a very complex process, the brain may be using fairly basic, preexisting computational methods.[13]
Clinical significance
Aphasia
Wernicke's area is named after Carl Wernicke, a German neurologist and psychiatrist who, in 1874, hypothesized a link between the left posterior section of the superior temporal gyrus and the reflexive mimicking of words and their syllables that associated the sensory and motor images of spoken words.[14] He did this on the basis of the location of brain injuries that caused aphasia. Receptive aphasia in which such abilities are preserved is also known as Wernicke's aphasia. In this condition there is a major impairment of language comprehension, while speech retains a natural-sounding rhythm and a relatively normal syntax. Language as a result is largely meaningless (a condition sometimes called fluent or jargon aphasia).
Wernicke’s area receives information from the auditory cortex, and functions to assign word meanings. [15] This is why damage to this area results in meaningless speech, often with paraphasic errors and newly created words or expressions. Paraphasia can involve substituting one word for another, known as semantic paraphasia, or substituting one sound or syllable for another, defined as phonemic paraphasia.[16] This speech is often referred to as “word salad,” as speech sounds fluent but does not have sensible meaning. Normal sentence structure and prosody are preserved, with normal intonation, inflection, rate ,and rhythm.[16] This differs from Broca’s aphasia, which is characterized by nonfluency. Patients are typically not aware that their speech is impaired in this way, as they have altered comprehension of their speech. Written language, reading, and repetition are affected as well. [15] [16]
Damage to the posterior temporal lobe of the dominant hemisphere is the cause of Wernicke’s aphasia. [16] The etiology of this damage can vary greatly, with the most common cause being a cerebrovascular event such as an ischemic stroke. Ischemic stroke is the result of a thrombus occluding a blood vessel, restricting blood supply to a particular area of the brain. Other causes of focal damage potentially leading to Wernicke’s aphasia include head trauma, infections affecting the central nervous system, neurodegenerative disease, and neoplasms. [16] A cerebrovascular event is more likely the cause in an acute-onset presentation of aphasia, whereas a degenerative disease should be suspected in aphasia with gradual progression over time. [15] Imaging is often useful in identifying a lesion, with most common initial imaging consisting of computed tomography (CT) scan or magnetic resonance imaging (MRI). [17] Electroencephalography (EEG) can also be useful in patients with transient aphasia, where findings may be due to seizures, although this is a less common cause. [15]
Diagnosis of aphasia, as well as characterization of type of aphasia, is done with language testing by the provider. Testing should evaluate fluency of speech, comprehension, repetition, ability to name objects, and writing skills. [16] Fluency is assessed by observing the patient’s spontaneous speech. Abnormalities in fluency would include shortened phrases, decreased number of words per minute, increased effort with speech, and agrammatism. [15] Patients with Wernicke’s aphasia should have fluent speech, so abnormalities in fluency may indicate a different type of aphasia. Comprehension is assessed by giving the patient commands to follow, beginning with simple commands and progressing to more complex commands. Repetition is evaluated by having the patient repeat phrases, progressing from simple to more complex phrases. [15] Both comprehension and repetition would be abnormal in Wernicke’s aphasia. Content should also be assessed, by listening to a patient’s spontaneous or instructed speech. Content abnormalities include paraphasic errors and neologisms, both indicative of a diagnosis of Wernicke’s aphasia. [15] A full neurologic exam should also be done, which will help differentiate aphasia from other neurologic diagnoses potentially causing altered mental status with abnormal speech and comprehension. [15]
Treatment of Wernicke’s aphasia first involves addressing the underlying cause. Speech and language therapy is the first line treatment for the aphasia itself, and has a goal of improving language deficits as well as preserving the patient’s remaining language skills. [16] A subsequent critical goal of therapy is to teach the patient how to communicate in alternative ways, so they can successfully communicate in daily life. [16] This may include gestures, pictures, or use of electronic devices. [17]
While neuroimaging and lesion evidence generally support the idea that malfunction of or damage to Wernicke's area is common in people with receptive aphasia, this is not always so. Some people may use the right hemisphere for language, and isolated damage of Wernicke's area cortex (sparing white matter and other areas) may not cause severe receptive aphasia.[3][18] Even when patients with Wernicke's area lesions have comprehension deficits, these are usually not restricted to language processing alone. For example, one study found that patients with posterior lesions also had trouble understanding nonverbal sounds like animal and machine noises.[19] In fact, for Wernicke's area, the impairments in nonverbal sounds were statistically stronger than for verbal sounds.
References
- "Aphasia: Signs & Symptoms". American Speech-Language-Hearing Association.
- Kennison, Shelia (2013). Introduction to language development. Los Angeles: Sage.
- Bogen JE, Bogen GM (1976). "Wernicke's region—Where is it?". Annals of the New York Academy of Sciences. 280 (1): 834–43. Bibcode:1976NYASA.280..834B. CiteSeerX 10.1.1.657.3681. doi:10.1111/j.1749-6632.1976.tb25546.x. PMID 1070943.
- Nakai, Y; Jeong, JW; Brown, EC; Rothermel, R; Kojima, K; Kambara, T; Shah, A; Mittal, S; Sood, S; Asano, E (2017). "Three- and four-dimensional mapping of speech and language in patients with epilepsy". Brain. 140 (5): 1351–1370. doi:10.1093/brain/awx051. PMC 5405238. PMID 28334963.
- Démonet JF, Chollet F, Ramsay S, Cardebat D, Nespoulous JL, Wise R, Rascol A, Frackowiak R (December 1992). "The anatomy of phonological and semantic processing in normal subjects". Brain. 115 (Pt 6): 1753–68. doi:10.1093/brain/115.6.1753. PMID 1486459.
- DeWitt I, Rauschecker JP (2012). "Phoneme and word recognition in the auditory ventral stream". Proceedings of the National Academy of Sciences. 109 (8): E505–E514. Bibcode:2012PNAS..109E.505D. doi:10.1073/pnas.1113427109. PMC 3286918. PMID 22308358.
- DeWitt I, Rauschecker JP (2013). "Wernicke's area revisited: parallel streams and word processing". Brain Lang. 127 (2): 181–91. doi:10.1016/j.bandl.2013.09.014. PMC 4098851. PMID 24404576.
- Mesulam MM (June 1998). "From sensation to cognition". Brain. 121 (Pt 6): 1013–52. doi:10.1093/brain/121.6.1013. PMID 9648540.
- Bernal B, Ardila A (September 2009). "The role of the arcuate fasciculus in conduction aphasia". Brain. 132 (Pt 9): 2309–16. doi:10.1093/brain/awp206. PMID 19690094.
- Saur D, Kreher BW, Schnell S, Kümmerer D, Kellmeyer P, Vry MS, Umarova R, Musso M, Glauche V, Abel S, Huber W, Rijntjes M, Hennig J, Weiller C (November 2008). "Ventral and dorsal pathways for language". Proceedings of the National Academy of Sciences. 105 (46): 18035–18040. Bibcode:2008PNAS..10518035S. doi:10.1073/pnas.0805234105. PMC 2584675. PMID 19004769.
- Harpaz Y, Levkovitz Y, Lavidor M (October 2009). "Lexical ambiguity resolution in Wernicke's area and its right homologue". Cortex. 45 (9): 1097–103. doi:10.1016/j.cortex.2009.01.002. PMID 19251255.
- Poeppel D, Idsardi WJ, van Wassenhove V (March 2008). "Speech perception at the interface of neurobiology and linguistics". Philosophical Transactions of the Royal Society B. 363 (1493): 1071–86. doi:10.1098/rstb.2007.2160. PMC 2606797. PMID 17890189.
- Newman AJ, Supalla T, Hauser P, Newport EL, Bavelier D (2010). "Dissociating neural subsystems for grammar by contrasting word order and inflection". Proceedings of the National Academy of Sciences. 107 (16): 7539–44. Bibcode:2010PNAS..107.7539N. doi:10.1073/pnas.1003174107. PMC 2867749. PMID 20368422.
- Wernicke K. (1995). "The aphasia symptom-complex: A psychological study on an anatomical basis (1875)". In Paul Eling (ed.). Reader in the History of Aphasia: From sasi(Franz Gall to). 4. Amsterdam: John Benjamins Pub Co. pp. 69–89. ISBN 978-90-272-1893-3.
- Glenn Clark, David (2018). "Approach to the patient with aphasia". Up To Date.
- B. Acharya, Aninda. "Wernicke Aphasia". National Center for Biotechnology Information.
- "Aphasia". National Institute on Deafness and Other Communication Disorders. March 6, 2017.
- Dronkers NF.; Redfern B B.; Knight R T. (2000). "The neural architecture of language disorders". In Bizzi, Emilio; Gazzaniga, Michael S. (eds.). The New cognitive neurosciences (2nd ed.). Cambridge, Massachusetts: MIT Press. pp. 949–58. ISBN 978-0-262-07195-6.
- Saygin AP, Dick F, Wilson SM, Dronkers NF, Bates E (2003). "Neural resources for processing language and environmental sounds: evidence from aphasia". Brain. 126 (Pt 4): 928–45. doi:10.1093/brain/awg082. PMID 12615649.
External links
