Strabismus surgery
Strabismus surgery (also: extraocular muscle surgery, eye muscle surgery, or eye alignment surgery) is surgery on the extraocular muscles to correct strabismus, the misalignment of the eyes. With approximately 1.2 million procedures each year, extraocular muscle surgery is the third most common eye surgery in the United States.[1] The earliest successful strabismus surgery intervention is known to have been performed on 26 October 1839 by Johann Friedrich Dieffenbach on a 7-year-old esotropic child; a few earlier attempts had been performed in 1818 by William Gibson of Baltimore, a general surgeon and professor at the University of Maryland.[2]
| Strabismus surgery | |
|---|---|
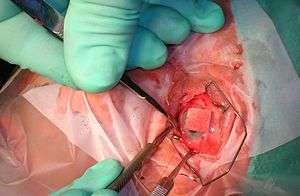 Isolating the inferior rectus muscle | |
| Specialty | ophthalmology |
The idea of treating strabismus by cutting some of the extraocular muscle fibers was published in American newspapers by New York oculist John Scudder in 1837[3]
Types
- Eye muscle surgeries typically correct strabismus and include the following:[4][5]
- Loosening / weakening procedures
- Recession involves moving the insertion of a muscle posteriorly towards its origin.
- Myectomy
- Myotomy
- Tenectomy
- Tenotomy
- Tightening / strengthening procedures
- Resection involves detaching one of the eye muscles, removing a portion of the muscle from the distal end of the muscle and reattaching the muscle to the eye.[6]
- Tucking
- Advancement is the movement of an eye muscle from its original place of attachment on the eyeball to a more forward position.
- Transposition / repositioning procedures
- Adjustable suture surgery is a method of reattaching an extraocular muscle by means of a stitch that can be shortened or lengthened within the first post-operative day, to obtain better ocular alignment.[7][8]
- Loosening / weakening procedures
Strabismus surgery is a one-day procedure. The patient spends only a few hours in the hospital with minimal preoperative preparation. The average duration of the surgery is variable. After surgery, the patient should expect soreness and redness. In cases of re-operations, more pain is expected. Resection of the muscles is more painful in the post operative period than recession. It also leaves redness that lasts longer and may cause some vomiting in the early post operative period.
The surgeon will provide the patient with a cover for his or her eyes that prevents light from entering. It is advisable for the patient to wear this, since stimulus to the eye (e.g., light, rolling of eyes) will cause discomfort.
Outcomes
Alignment and functional changes
Over- and undercorrection: Surgical intervention can result in the eyes being entirely aligned (orthophoria) or nearly so, or it can result in an over- or undercorrection that may necessitate further treatment or another surgical intervention. The likelihood that the eyes will stay aligned over the longer term is higher if the patient is able to achieve some degree of binocular fusion after surgery than if not. In a study on infantile esotropia patients who had either small-angle (8 diopters) esotropia or small-angle exotropia of the same size six months after the intervention, it was found that those who had the small-angle esotropia were more likely to have aligned eyes five years after the intervention than those with small-angle exotropia.[9] There is tentative evidence that children with infantile esotropia patients achieve better binocular vision post-operatively if the surgical treatment is performed early (see: Infantile esotropia#Surgery).
Other deviations: Strabismus surgery for oblique muscle disorders may result in consecutive misalignment of the eyes. First of all, dissociated vertical deviation may occur. There are indications that the severity of this deviation may be lower if a child is operated at a very young age.[10] Secondly, strabismus surgery may also result in subjective and objective cyclodeviation, possibly resulting in cyclotropia and rotational double vision (cyclodiplopia) if the visual system cannot compensate for it.[11][12]
For pure horizontal rectus muscle surgeries, it is known that vertical deviations, A and V patterns and cyclotropia can be anticipated or avoided by taking certain surgical precautions.[13]
Functional considerations: A frequent outcome of strabismus surgery is consecutive microtropia (also known as monofixation syndrome).[14]
Functional improvements and further benefits: For a long time it was thought that adult patients with long-standing strabismus could achieve only cosmetic improvement; in recent years there have been cases in which sensory fusion has occurred also in this type of patients provided that postoperative motor alignment is very high.[15] In case of pre-operative inward squint the correction expands the binocular visual field of the patient, improving peripheral vision. Furthermore, the restoration of ocular alignment can bring about psychosocial and economic benefits to the patient (see also: Psychosocial effects of strabismus).[15]
Complications
Diplopia occurs rather frequently in the first few weeks following surgery.
Complications that occur rarely or very rarely following surgery include: eye infection, hemorrhage in case of scleral perforation, muscle slip or detachment, or even loss of vision.
Eye muscle surgery gives rises to scarring (fibrosis); if scarring is extensive, it may be seen as raised and red tissue on the white of the eye. Fibrosis can be reduced by use of mitomycin C during surgery.[16]
A relatively new method, primarily devised by Swiss ophthalmologist Daniel Mojon, is minimally invasive strabismus surgery (MISS)[17][18]which has the potential to reduce the risk of complications and lead to faster visual rehabilitation and wound healing. Done under the operating microscope, the incisions into the conjunctiva are much smaller than in conventional strabismus surgery. A study published in 2017 documented fewer conjunctival and eyelid swelling complications in the immediate postoperative period after MISS with long-term results being similar between both groups.[19] MISS can be used to perform all types of strabismus surgery, namely rectus muscle recessions, resections, transpositions, and plications even in the presence of limited motility.[20]
Very rarely, potentially life-threatening complications may occur during strabismus surgery due to the oculocardiac reflex.
See also
References
- Hertle, Richard. "Eye Muscle Surgery and Infantile Nystagmus Syndrome" (Microsoft Word document). American Nystagmus Network. Retrieved 2006-10-10.
- Gunter K. von Noorden: Binocular Vision and Ocular Motility: Theory and management of strabismus, Chapter 26: Principles of Surgical Treatment, telemedicine.orbis.org
- Leffler CT, Schwartz SG, Le JQ (2017). "American Insight into Strabismus Surgery before 1838". Ophthalmology and Eye Diseases. 9: 1179172117729367. doi:10.1177/1179172117729367. PMC 5598791. PMID 28932129.
- Surgery Encyclopedia - Eye Muscle Surgery
- Strabismus Surgery
- Strabismus.com - Strabismus Surgery
- Parikh, RK; Leffler, CT (July 2013). "Loop suture technique for optional adjustment in strabismus surgery". Middle East African Journal of Ophthalmology. 20 (3): 225–228. doi:10.4103/0974-9233.114797. PMC 3757632. PMID 24014986.
- Eye Procedures > Adjustable Suture Strabismus Surgery - EyeMDLink.com Archived 2005-12-27 at the Wayback Machine
- Kushner BJ1 Fisher M (1996). "Is alignment within 8 prism diopters of orthotropia a successful outcome for infantile esotropia surgery?". Arch Ophthalmol. 114 (2): 176–180. doi:10.1001/archopht.1996.01100130170010. PMID 8573021.
- Yagasaki, T.; Yokoyama, Y. O.; Maeda, M. (Jul 2011). "Influence of timing of initial surgery for infantile esotropia on the severity of dissociated vertical deviation". Jpn J Ophthalmol. 55 (4): 383–388. doi:10.1007/s10384-011-0043-1. PMID 21647566.
- See section "Discussion" in: Pradeep Sharma; S. Thanikachalam; Sachin Kedar; Rahul Bhola (January–February 2008). "Evaluation of subjective and objective cyclodeviation following oblique muscle weakening procedures". Indian Journal of Ophthalmology. 56 (1): 39–43. doi:10.4103/0301-4738.37594. PMC 2636065. PMID 18158402.
- H. D. Schworm; S. Eithoff; M. Schaumberger; K. P. Boergen (February 1997). "Investigations on subjective and objective cyclorotatory changes after inferior oblique muscle recession". Investigative Ophthalmology & Visual Science. 38 (2). pp. 405–412.
- Khawam, E.; Jaroudi, M.; Abdulaal, M.; Massoud, V.; Alameddine, R.; Maalouf, F. (2013). "Major review: Management of strabismus vertical deviations, A- and V-patterns and cyclotropia occurring after horizontal rectus muscle urgery with or without Oblique Muscle Surgery". Binocul Vis Strabolog Q Simms Romano. 28 (3): 181–192. PMID 24063512.
- Guthrie, ME; Wright, KW (September 2001). "Congenital esotropia". Ophthalmol Clin North Am. 14 (3): 419–24, viii. doi:10.1016/S0896-1549(05)70239-X. PMID 11705141.
- Edelman PM (2010). "Functional benefits of adult strabismus surgery". Am Orthopt J. 60 (60): 43–47. doi:10.3368/aoj.60.1.43. PMID 21061883.
- Kersey, J. P.; Vivian, A. J. (Jul–Sep 2008). "Mitomycin and amniotic membrane: a new method of reducing adhesions and fibrosis in strabismus surgery". Strabismus. 16 (3): 116–118. doi:10.1080/09273970802405493. PMID 18788060.
- Mojon DS: Minimally invasive strabismus surgery. In: Eye. (Lond). 29, 2015, S. 225–233.
- Mojon DS: Comparison of a new, minimally invasive strabismus surgery technique with the usual limbal approach for rectus muscle recession and plication. In: Br J Ophthalmol. 91, 2007: 76–82.
- Gupta P, Dadeya S, Kamlesh, Bhambhawani V: Comparison of Minimally Invasive Strabismus Surgery (MISS) and Conventional Strabismus Surgery Using the Limbal ApproachJ Pediatr Ophthalmol Strabismus. 2017;54:208-215..
- Asproudis I, Kozeis N, Katsanos A, Jain S, Tranos PG, Konstas AG : A Review of Minimally Invasive Strabismus Surgery (MISS): Is This the Way Forward? Adv Ther. 2017;34:826-833.
Further reading
- Wright, Kenneth W.; Thompson, Lisa S.; Strube, Yi Ning; Coats, David K. (August 2014). "Novel strabismus surgical techniques—not the standard stuff". Journal of American Association for Pediatric Ophthalmology and Strabismus (JAAPOS). 18 (4): e47. doi:10.1016/j.jaapos.2014.07.152.
- Kushner, Burton J. (2014). "The Benefits, Risks, and Efficacy of Strabismus Surgery in Adults". Optometry and Vision Science. 91 (5): e102–e109. doi:10.1097/OPX.0000000000000248. ISSN 1040-5488. PMID 24739461.
- Engel JM (September 2012). "Adjustable sutures: an update". Current Opinion in Ophthalmology. 23 (5): 373–6. doi:10.1097/ICU.0b013e3283567321. PMID 22871879.
External links
- Strabismus Surgery, Horizontal on EyeWiki from the American Academy of Ophthalmology
- Strabismus Surgery Complications on EyeWiki from the American Academy of Ophthalmology