Rectal foreign body
Rectal foreign bodies are large foreign items found in the rectum that can be assumed to have been inserted through the anus, rather than reaching the rectum via the mouth and gastrointestinal tract. It can be of clinical relevance if the patient cannot remove it the way they intended. Smaller, ingested foreign bodies, such as bones eaten with food, can sometimes be found stuck in the rectum upon x-ray and are rarely of clinical relevance.
| Rectal foreign body | |
|---|---|
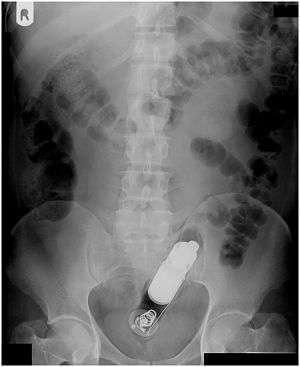 | |
| Radiograph of a male abdomen with a vibrator inside the rectum | |
| Specialty | Emergency medicine, general surgery |
Rectal foreign bodies are a subgroup of foreign bodies in the alimentary tract.[1][2]
Signs and symptoms
If the foreign body is too big to allow feces from the colon to pass, a mechanical ileus may occur. The distension of the rectum and the disruption of the peristasis reinforce this effect.
The foreign body may cause infections, destroying the intestinal wall. Depending on the location of the perforation, this may lead to a peritonitis due to the feces or an abscess in the retroperitoneal space.
Smaller objects that injure the intestinal wall, but do not perforate it, may be encapsulated by a foreign body granuloma. They may remain in the rectum as a pseudotumor without any further effects.
Complications
The most common – but still rare – complication is a perforation of the rectum caused by the foreign object itself or attempts to remove it. Diagnosed perforations are operated immediately by opening the abdomen and removal or suturing of the perforated area. In order to suppress infections, antibiotics are usually prescribed.[3] Often, a temporary ileostomy is necessary to protect the stitches.[4] After a contrast medium applied by an enema proves the complete healing of the perforated area, the ileostomy is reversed. This usually takes between three and six months. [5] Average hospitalization is 19 days.[3]
Medical literature describes some deaths due to rectal foreign bodies, but they are very rare and usually classified as autoerotic fatality. A 75-year-old patient died due to a rectal perforation caused by a mentally ill person using a cane.[6] Another middle-aged patient died due to a rectal perforation by a vibrator. The perforation was sutured and the patient received intensive medical care, but he contracted Acute Respiratory Distress Syndrome (ARDS) and systemic inflammatory response syndrome (SIRS) due to the trauma, resulting in multiple organ dysfunction syndrome (MODS) and death.[7] There is a paper describing a death after a perforation with a shoehorn.[8] The rectum has to be nursed after a surgical procedure until healing is complete. A 54-year-old man, who had been operated on twice in order to remove a foreign body (a cucumber and a parsnip), died due to a peritonitis after he inserted two apples into the rectum before the wound had healed.[9]
Causes
Reasons for foreign rectal bodies vary wildly, but in most cases they are of sexual or criminal motivation.[10] The foreign body was inserted voluntarily in the vast majority of cases. This especially includes sexually motivated behaviour, encompassing the majority of cases. Bodypacking, i.e. illegal transport of drugs within a body orfice (here: inside the rectum), is another – potentially – voluntary reason for insertion of foreign rectal bodies.[11] This includes attempts to transport objects like weapons, including knives, or ammunition. According to one study, sexual stimulation was responsible for 80% of clinically relevant foreign rectal bodies. About 10% of the cases were due to sexual assault.[4]
In rare cases, the patient inserted the object into the rectum without a way to remove it intending to receive attention and pity from doctors and nurses. This behaviour is categorized as Munchausen's syndrome.[12]
Another cause may be attempted self-treatment of diseases. One patient attempted to treat his chronic diarrhea by inserting an ear of maize into his rectum.[13] Another patient tried to soothe the itching due to his hemorrhoids (Pruritus ani) with a toothbrush. The toothbrush went out of control and disappeared inside his anus.[14]
Accidents or torture may cause an involuntary insertion of a foreign body.[15] A mercury medical thermometer inserted into the anus in order to measure the temperature, but broke off while inside, is an example of a foreign rectal body due to an accident.[16] Ancient Greece knew the Rhaphanidosis as a punishment for male adulterers. It involved the insertion of a radish into the anus. Many self-inserted rectal bodies are stated as accidentally by the patients due to feelings of shame.
There are several reasons that contribute to the jamming of rectal bodies inside the rectum. Many of the objects used for sexual stimulation have a conical tip in order to facilitate penetration, while the base is flat. Extraction by the user may be impossible if the base of the object passed the anus towards the rectum. In order to receive a stronger stimulation, the object may be inserted deeper than intended. In this case, the sphincter prevents, by mechanical means, the extraction of the foreign body.[3]
By mouth
The other way for a foreign body to travel through the digestive system (after oral intake and passage through the entire intestines) happens very often, but is only rarely medically relevant. Other constriction, such as the esophagus, cardia, pylorus or ileocecal valve tend to cause issues with other organs, provided a foreign body is large enough to be an issue. Some foreign bodies may still pass those narrows and may cause medically relevant issues, i.e. toothpicks and bones.[2][17] Bones especially, i.e. from chickens, cause about half of all intestinal perforations.[18][19]
Plant-based food, especially seeds like popcorn,[20] watermelon, sunflower and pumpkin seed, may clump together inside the lower intestines to form bezoars. Those may grow too big for normal anal passage, thus becoming clinically relevant. This kind of rectal foreign body happens chiefly in children, especially in Northern Africa and the Middle East, where those seeds form an elemental part of the diet.[21][22] In very rare cases, seeds inside a bezoar may germinate inside the lower intestines or the rectum, causing a blockade.[23]
Objects
Type and size of the foreign rectal bodies are diverse and may exceed the anatomical-physiological imagination.[10]
Objects documented in literature include:
- Razor, screw, screwdriver, small rolled tool bag (15×12 cm, including tools 620 g), hairpin, milk can opener
- Short staffs, such as a 27 cm long chair leg, a 19 cm long spade handle and a broken off broom handle, extension parts for a vacuum cleaner
- Containers, sometimes exceeding 0.5 l in volume, e.g. sparkling wine bottles, bottles of Coca-Cola, jam pots, small beer glasses, cups
- Spray can, light bulb, vacuum tube, candle
- Table tennis ball, Boccia ball
- Ammunition, firecracker
- Vibrator, rubber rod, dildo
- a toy car
- spectacles, a suitcase key, a tobacco pouch and a magazine at the same time
- plastic tooth brush case[10][3][9][24][25][26]
Not all objects are solid. In 1987, a case was documented of a patient who administered a cement enema. After it solified and impacted, the resulting block had to be surgically extracted.[27] Another extreme case occurred in November 1953. A depressed man inserted a 15 cm long cardboard tube into his rectum and tossed a lighted firecracker into the tube's opening, resulting in a large hole in his rectum.[28]
Diagnosis
Many patients feel ashamed during the anamnesis and provide information only reluctantly. This may lead to missing information that may be important during therapy. For the same reason, patients may not visit a doctor until very late. Trusting and sensitive care for the ashamed and uncomfortable patients is paramount for a successful therapy[29] and may be life-saving.[30]
Usually, several radiological images are recorded in order to pinpoint the precise place and depth of the foreign body. This is usually done by x-ray. Foreign bodies made from low-contrast material (e.g. plastics) may necessitate medical ultrasound or a CT scan.[29] Magnetic resonance imaging is contraindicated, especially if the foreign body is unknown. Foreign rectal bodies may penetrate deep into the colon, in certain circumstances up to the right colic flexure.[10]
An endoscopy, which may also be of use during therapy, facilitates the identification and localisation of the object inside the rectum.[31]
Information about the foreign body obtained in those ways are of high importance during therapy, as a perforation of the rectum or the anus is to be absolutely avoided.
Treatment

The therapeutic measures to remove the foreign body can be as diverse as the objects inside the rectum. In many instances, the foreign bodies consist of fragile materials, such as glass. Most patients wait for several hours or even days until they visit a doctor. Before they do, they often repeatedly try to remove the object themselves or by a layperson. This often worsens the situation for a successful extraction.
In most cases, the foreign body can be removed endoscopic. Vibrators, for example, can be often removed using a large sling usually used to remove polyps during coloscopy.[32] Smaller objects like a medical thermometer can be removed by a biopsy forceps.[33] A flexible endoscope can be of no help with large and jammed objects. It may be preferable to use rigid tools in those cases.[10]
There have been several cases where instruments used in child birth have proven their worth for the removal of those foreign bodies, such as the forceps[34] and suction cups.[35] Wooden objects have been retrieved with corkscrews and drinking glasses after filling them with plaster.[34][36] A spoon can be used as an "anchor" by leaving it inside the glass during the plaster filling, removing it together with the glass.[9] Light bulbs are encased in a gauze shroud, shattered inside the rectum and extracted.[9]
There have been successful cases using argon-plasma coagulation. The object in question was a green apple wrapped in cellophane inside the rectum of a 44-year-old patient. The argon-beam coagulation shrunk the apple by more than 50%, enabling its removal. Previous extraction attempts using endoscopic tools failed due to the flat surface of the object.[37]
If the object is too far up, in the area of the colon sigmoideum, and cannot be removed using one of the above methods, bed rest and sedation can cause the object to descend back into the rectum, where retrieval and extraction are easier.[3]
In difficult cases, a laparotomy may be necessary. Statistically, this is the case in about 10 percent of patients.[10] The large intestine can be manipulated inside the abdominal cavity, making it possible for it to wander in the direction of the anus and be grabbed there. A surgical opening of the large intestines can be indication in very difficult cases, especially if the manipulation of the object may pose a serious health risk. This may be the case with a jammed drug condom.[31]
Anaesthesia
Mild cases may need a sedation at most. Local and spinal anaesthesia find common use. Difficult interventions may need general anaesthesia; surgical opening of the abdominal cavity or the colon require it. General anaesthesia can be beneficial for the relaxation of the sphincter.[10]
Aftercare
After the surgery, a sigmoidoscopy – a colonoscopy focused on the first 60 cm of the colon – is good practice in order to rule out possible perforation and injury of the rectum and the colon sigmoideum.[38] Stationary aftercare may be indicated.
Examples
| Object | Procedure | Anaesthesia | Source |
|---|---|---|---|
| Ball pen | Polypectomy sling | N.A. | [39] |
| Water-filled balloon | Punction | N.A. | [40] |
| Chicken bone | Polypectomy sling | N.A. | [41] |
| Toothpick | Polypectomy sling | N.A. | [42] |
| Apple in cellophane | Defragmentation using APC | none | [37] |
| Glass bottle | Biopsy forceps | General anaesthesia | [33] |
| Vibrator | Polypectomy sling | none | [33] |
| Vial | Sengstaken–Blakemore tube | N.A. | [43] |
| Vial | Polypectomy sling | N.A. | [44] |
| Enema tip | Polypectomy sling | N.A. | [44] |
| Vibrator | Biopsy forceps | N.A. | [44] |
| Pencil | Polypectomy sling | N.A. | [45] |
| Iron rod | Two-channel endoscope and wires | N.A. | [46] |
| Bottleneck | Foley catheter | General anaesthesia | [47] |
| Spray tank | Achalasy balloon | None | [38] |
| Sponge-like toy ball | Suction cup | General anaesthesia | [48] |
| Vibrator | Forceps and anal dilation | Local anaesthesia | [49] |
| Vibrator | Hooked tongs | Local anaesthesia | [50] |
| Bottle of aftershave | Bone holding forceps with rubber feet | Spinal anaesthesia | [51] |
| Chicken bones | Fingers | None | [18] |
| Aerosol-can cap | Grasping forceps and anal dilation | General anaesthesia | [52] |
| Vase | Filling with plaster | General anaesthesia | [53] |
| Glass container | Extraction using plaster | Spinal anaesthesia | [54] |
| Glass container | Tracheal tube | Local anaesthesia | [55] |
| Apple | Two-handed manipulation | Local anaesthesia | [56] |
| Glass container | Foley catheter | General anaesthesia | [57] |
| Glass bottle | Suction cup | General anaesthesia | [29] |
| 100-watt electric bulb | Three Foley catheters | N.A. | [58] |
| Thermometer | Biopsy forceps | General anaesthesia | [33] |
| Vibrator | transanal Kocher's forceps | Local anaesthesia | [33] |
| Bowling bottle (Bottle in the shape of a pin) | Forceps | General anaesthesia | [33] |
| Perfume bottle | manual | Spinal anaesthesia | [59] |
| Piece of wood | manual | General anaesthesia | [60] |
| Toothbrush container | Fogarty catheter | N.A. | [61] |
| Oven mitt | Forceps, after anal dilation | General anaesthesia | [62] |
| Drainpipe | forceps in childbirth | General anaesthesia | [34] |
| Pétanque ball | Electromagnet | General anaesthesia | [63] |
| Carrot | Myoma lifter | N.A. | [64] |
| Glass object | Suction cup | Spinal anaesthesia | [35] |
| Rubber ball | manual extraction after anal dilation | General anaesthesia | [65] |
| Wooden staff | Two-handed anal dilation | Spinal anaesthesia | [65] |
| Bottle | manual after anal dilation | General anaesthesia | [66] |
| Dildo | Myoma lifter | N.A. | [67] |
| Light bulb | Abdominal compression | Spinal anaesthesia | [68] |
Daten nach[38]
- APC = Argon beam-coagulation
- N.A. = Not available
Epidemiology
There is no reliable data about the incidence of clinically meaningful foreign rectal bodies. It may have increased in the long term[17] as it is observed more often in recent times.[69]
The incident rate is significantly higher for men than for women. The gender ratio is in the area of 28:1.[17][70][71] A metastudy in the year 2010 found a ratio of 37:1. Median age of the patients was 44.1 years, with a standard deviation of 16.6 years.[72] Rectal foreign bodies are not an unusual occurrence in hospital emergency rooms.[73]
The first documented case dates from the 16th century.[12][74]
Other animals
Foreign rectal bodies are rare in veterinary medicine. A passage through the entire intestines, followed by a stay inside the rectum is – as with humans – rare.[75] Animals may have bezoars out of different materials, which may migrate to the rectum and cause problems.[76] Atypical foreign rectal bodies in animals of both sexes may be caused by sexual or sadistic abuse.[77]
Ig Nobel Prize
The Ig Nobel Prize was awarded in 1995 to David B. Busch and James R. Starling from Madison, Wisconsin for their 1986 article Rectal foreign bodies: Case Reports and a Comprehensive Review of the World’s Literature[59] (see List of Ig Nobel Prize winners).[78]
See also
- Đorđe Martinović incident
- Foreign body in alimentary tract
- Urethral foreign body insertion
- Butt plug
References
- A. A. Ayantunde, T. Oke: A review of gastrointestinal foreign bodies. In: Int J Clin Pract 60, 2006, S. 735–739. PMID 16805760 (Review)
- M. T. Smith, R. K. Wong: Foreign bodies. In: Gastrointest Endosc Clin N Am 17, 2007, S. 361–382. PMID 17556153 (Review)
- J. E. Barone u. a.: Perforations and foreign bodies of the rectum: report of 28 cases. In: Ann Surg 184, 1976, S. 601–604. PMID 984928
- J. S. Cohen and J. M. Sackier: Management of colorectal foreign bodies. In: J Roy Coll Surg Edin 41, 1996, S. 312–315. PMID 8908954
- J. Ruiz del Castillo u. a.: Colorectal trauma caused by foreign bodies introduced during sexual activity: diagnosis and management. In: Rev Esp Enferm Dig 93, 2001, S. 631–634. PMID 11767487 (Review)
- N. Ikeda u. a.: Homicide by rectal insertion of a walking stick. In: Nihon Hoigaku Zasshi. Band 45, 1991, S. 341–344. PMID 1766149
- N. G. Waraich u. a.: Vibrator-induced fatal rectal perforation. In: New Zealand Medical Journal. Band 120, 2007, S. U2685. PMID 1772649.
- R. W. Byard u. a.: Unusual fatal mechanisms in nonasphyxial autoerotic death. In: Am Journal of Forensic Medical Pathology. Band 21, 2000, S. 65–68. PMID 10739230
- "Sturz in die Kiste", Der Spiegel, 7 October 1991 (41), pp. 317–320, 1991
- H. Messmann: Lehratlas der Koloskopie. Georg Thieme Verlag, 2004, ISBN 3-13-136441-6, S. 219. ISGN , p. 219, at Google Books
- M. C. Laitenberger: Klinische und rechtsmedizinische Aspekte des intestinalen Rauschmitteltransportes in Hamburg 1989 bis 2004. Dissertation, Universität Hamburg, 2005.
- S. A. Khan u. a.: Munchausen's syndrome presenting as rectal foreign body insertion: a case report. In: Cases J 1, 2008, 243. PMID 18925957 (Open Access)
- V. Stenz u. a.: Fremdkörpergeschichten. In: Ther Umsch 65, 2008, S. 699–702. PMID 19048523
- M. Kumar (July 2001). "Don't forget your toothbrush!". British Dental Journal. 191 (1): 27–28. doi:10.1038/sj.bdj.4801082a. ISSN 0007-0610. PMID 11491473.
- F. Nuschler u. a.: Bericht über die internationale Folterfoschung. (PDF; 4,6 MB) Universität Duisburg, 1992.
- B. Azman; B. Erku; B. H. Güvenç (May 2009). "Balloon extraction of a retained rectal foreign body under fluoroscopy, case report and review". Pediatric Emergency Care. 25 (5): 345–347. doi:10.1097/PEC.0b013e3181a3494f. ISSN 1535-1815. PMID 19444034.
- D. W. Munter: Foreign Bodies, Rectum. Vom 28. September 2009, abgerufen am 15. April 2010.
- D. H. Davies: A chicken bone in the rectum. In: Arch Emerg Med 8, 1991, S. 62–64. PMID 1854398
- J. E. Manus: Perforation of the intestine by ingested foreign bodies. In: American Journal of Surgery 53, 1941, S. 392–397.
- R. J. Roberge u. a.: Popcorn primary colonic phytobezoar. In: Ann Emerg Med 17, 1988, S. 77–79. PMID 3337421
- A. Eitan u. a.: Fecal impaction in children: report of 53 cases of rectal seed bezoars. In: J Pediatr Surg 42, 2007, S. 1114–1117. PMID 17560231
- M. S. Mirza u. a.: Rectal bezoars due to pumpkin seeds. In: Trop Doct 39, 2009, S. 54–55. PMID 19211433.
- F. Mahjoub u. a.: Invading plant material appearing as a colonic tumoural mass in a four-year-old girl. In: Trop Doct 39, 2009, S. 253–254. PMID 19762589.
- Busch, D. B.; Starling, J. R. (1986). "Rectal foreign bodies: case reports and a comprehensive review of the world's literature". Surgery. 100 (3): 512–519. PMID 3738771.
- Akhtar, M.; Arora, P. (2009). "Case of unusual foreign body in the rectum". Saudi Journal of Gastroenterology. 15 (2): 131–132. doi:10.4103/1319-3767.48973. PMC 2702971. PMID 19568580.
- Khan, S. A.; Davey, C. A.; Khan, S. A.; Trigwell, P. J.; Chintapatla, S (2008). "Munchausen's syndrome presenting as rectal foreign body insertion: A case report". Cases Journal. 1 (1): 243. doi:10.1186/1757-1626-1-243. PMC 2572607. PMID 18925957.
- P. J. Stephens, M. L. Taff: Rectal impaction following enema with concrete mix. In: Am J Forensic Med Pathol 8, 1987, S. 179–182. PMID 3649167
- A. G. Butters: An unusual rectal injury. In: Br Med J 2, 1955, S. 602–603. PMID 13240191
- R. P. Mackinnon, G. Fulde: Removing rectal foreign bodies: is the ventouse gender specific? In: Med J Aust 169, 1998, S. 670–671. PMID 9887927
- E. Stein: Proktologie: Lehrbuch und Atlas. Verlag Springer, 2002, ISBN 3-540-43033-4, S. 329f. , p. 329, at Google Books
- A. T. R. Axon and M. Classen: Gastroenterologische Endoskopie. Georg Thieme Verlag, 2004, ISBN 3-13-132401-5, S. 400–401. , p. 400, at Google Books
- D. Hartmann u. a.: Notfallendoskopie – Update. In: Gastroenterologie up2date 5, 2009, S. 321–334. doi:10.1055/s-0029-1215318
- W. C. Huang u. a.: Retained rectal foreign bodies. In: J Chin Med Assoc 66, 2003, S. 607–612. PMID 14703278
- T. N. Peet: Removal of impacted rectal foreign body with obstetric forceps. In: British Medical Journal 1976, S. 500–501. PMID 1252815.
- S. O. Johnson and T. H. Hartranft: Nonsurgical removal of a rectal foreign body using a vacuum extractor. Report of a case. In: Dis Colon Rectum 39, 1996, S. 935–937. PMID 8756851
- H. Bailey and J. Love: A short textbook of surgery. A. J. H. Rains and H. D. Ritchie (Herausgeber), 16th edition. Verlag Lewis, 1975, S. 1013.
- J. Glaser u. a.: Unusual rectum foreign body: Treatment using argon-beam coagulation. (PDF; 224 kB) In: Endoscopy 29, 1997, S. 230–231. PMID 9201486.
- J. J. Koornstra and R. K. Weersma: Management of rectal foreign bodies: description of a new technique and clinical practice guidelines. Archived 2008-09-19 at the Wayback Machine In: World J Gastroenterol 14, 2008, S. 4403–4406. PMID 18666334
- R. M. Richter and L. M. Littman: Endoscopic extraction of an unusual colonic foreign body. In: Gastrointest Endosc 22, 1975, S. 40. PMID 1205104
- L. Wolf and K. Geraci: Colonscopic removal of balloons from the bowel. In: Gastrointest Endosc 24, 1977, S. 41. PMID 892400.
- P. R. Tarnasky u. a.: Colonoscopic diagnosis and treatment of chronic chicken bone perforation of the sigmoid colon. In: Gastrointest Endosc 40, 1994, S. 373–375. PMID 8056249
- H. H. Over u. a.: Toothpick impaction: treatment by colonoscopy. In: Endoscopy 29, 1997, S. S60–S61. PMID 9476787
- J. P. Hughes u. a.: Method of removing a hollow object from the rectum. In: Dis Colon Rectum 19, 1976, S. 44–45. PMID 1248348
- J. C. Kantarian u. a.: Endoscopic retrieval of foreign bodies from the rectum. In: Dis Colon Rectum 30, 1987, S. 902–904. PMID 3677968
- N. R. Vemula u. a.: Colonoscopic removal of a foreign body causing colocutaneous fistulas. In: Gastrointest Endosc 28, 1982, S. 195–196. PMID 7129050
- A. Ahmed and S. A. Cummings: Novel endoscopic approach for removal of a rectal foreign body. In: Gastrointest Endosc 50, 1999, S. 872–874 PMID 10570362
- D. Humes and D. N. Lobo: Removal of a rectal foreign body by using a Foley catheter passed through a rigid sigmoidoscope. In: Gastrointest Endosc 62, 2005, S. 610. PMID 16185979
- S. Feigelson u. a.: Removal of a large spherical foreign object from the rectum using an obstetric vacuum device: a case report. In: Am Surg 73, 2007, S. 304–306. PMID 17375796
- J. S. Haft u. a.: Vaginal vibrator lodged in rectum. In: Br Med J 1, 1976, S. 626. PMID 1252853.
- S. E: Levin u. a.: The use of a curved uterine vulsellum for removal of rectal foreign bodies: Report of a case. In: Diseases of the Colon & Rectum 20, 1977, S. 532–533. PMID 902553.
- D. Siroospour and L. R. Dragstedt: A large foreign body removed through the intact anus: report of a case. In: Dis Colon Rectum 18, 1975, S. 616–619. PMID 1181166.
- M. M. Aquino and J. W. Turner: A simple technique for removing an impacted aerosol-can cap from the rectum. In: Dis Colon Rectum 29, 1986, S. 675. PMID 3757713
- C. J. Couch u. a.: Rectal foreign bodies. In: Med J Aust 144, 1986, S. 512–515. PMID 3713565
- R. W. Graves u. a.: Anal eroticism: two unusual rectal foreign bodies and their removal. In: South Med J 76, 1983, S. 677–678. PMID 6844979
- H. I. Garber u. a.: Removal of a glass foreign body from the rectum. In: Dis Colon Rectum 24, 1981, S. 323. PMID 7238244
- H. Sharma u. a.: A novel technique for nonoperative removal of round rectal foreign bodies. In: Tech Coloproctol 11, 2007, S. 58–59. PMID 17357869
- M. Yaman u. a.: Foreign bodies in the rectum. In: Can J Surg 36, 1993, S. 173–177. PMID 8472230.
- V. S. Diwan: Removal of 100-watt electric bulb from rectum. In: Ann Emerg Med 11, 1982, S. 643–644. PMID 7137678
- D. B. Busch and J. R. Starling: Rectal foreign bodies: Case Reports and a Comprehensive Review of the World’s Literature. In: Surgery 100, 1986, S. 512–519. PMID 3738771
- A. A. Jansen: Foreign body in the rectum. In: N Z Med J 70, 1969, S. 174–175. PMID 5259744
- R. L. Wigle: Emergency department management of retained rectal foreign bodies. In: Am J Emerg Med 6, 1988, S. 385–389. PMID 3291887 (Review)
- J. E. Losanoff and K. T. Kjossev: Rectal "oven mitt": the importance of considering a serious underlying injury. In: J Emerg Med 17, 1999, S. 31–33. PMID 9950383
- C. J. Coulson u. a.: Extraction of a rectal foreign body using an electromagnet. In: Int J Colorectal Dis 20, 2005, S. 194–195. PMID 15322838.
- M. G. Vashist u. a.: Screwing a carrot out of the rectum. In: Indian J Gastroenterol 16, 1997, S. 120. PMID 9248200
- S. Nivatvongs u. a.: A simple technique to remove a large object from the rectum. In: J Am Coll Surg 203, 2006, S. 132–133. PMID 16798498
- S. Gopal: A bottle in the rectum. In: J Indian Med Assoc 62, 1974, S. 24–25. PMID 4839771
- S. K. Clark and N. D. Karanjia: A cork in a bottle – a simple technique for removal of a rectal foreign body. In: Ann R Coll Surg Engl 85, 2003, S. 282. PMID 12908471
- T. Konishi u. a.: Impaction of a rectal foreign body: what is the final approach before surgery? In: Dis Colon Rectum 50, 2007, S. 262–263. PMID 17164965
- N. Manimaran, M. Shorafa, J. Eccersley: Blow as well as pull: an innovative technique for dealing with a rectal foreign body. In: Colorectal disease: the official journal of the Association of Coloproctology of Great Britain and Ireland Band 11, No. 3, March 2009, S. 325–326, ISSN 1463-1318. doi:10.1111/j.1463-1318.2008.01653.x. PMID 18662236.
- D. L. Clarke u. a.: Colorectal foreign bodies. In: Colorectal Dis 7, 2005, S. 98–103. PMID 15606596
- L. B. Stack, D. W. Munter: Foreign bodies in the gastrointestinal tract. In: Emerg Med Clin North Am 14, 1996, S. 493–521. PMID 8681881 (Review)
- M. A. Kurer, C. Davey, S. Khan, S. Chintapatla: Colorectal foreign bodies: a systematic review. In: Colorectal disease: the official journal of the Association of Coloproctology of Great Britain and Ireland Band 12, No. 9, September 2010, S. 851–861, ISSN 1463-1318. doi:10.1111/j.1463-1318.2009.02109.x. PMID 19895597. (Review).
- Feigelson, S; Maun, D; Silverberg, D; Menes, T (2007). "Removal of a large spherical foreign object from the rectum using an obstetric vacuum device: A case report". The American Surgeon. 73 (3): 304–6. PMID 17375796.
- J. S. Haft, H. B. Benjamin: Foreign bodies in the rectum: some psychosexual aspects. In: Medical Aspects of Human Sexuality 7, 1973, S. 74–95.
- C. B. Webb u. a.: Rectal strictures in 19 dogs: 1997–2005. In: JAVMA. Band 43, 2007, S. 332–336. PMID 17975215
- N. D. Sargison u. a.: Intestinal obstruction in a blue-faced Leicester ram associated with a phytobezoar lodged at the pelvic inlet. In: Veterinary Record. Band 137, 1995, S. 222. PMID 7502475.
- H. M. C. Munro, M. V. Thrusfield: "Battered Pets": Sexual Abuse. In: Journal Of Small Animal Practice. Band 42, 2001, S. 333–337. PMID 11480898
- Improbable Research: Winners of the Ig® Nobel Prize.
External links
| Classification |
|---|
| Wikimedia Commons has media related to Rectal foreign bodies. |
- eMedicine gastrointestinal emergency medicine
- Medical Journal of Australia
- British Dental Journal case report: Don't forget your toothbrush! (subscribers only - with useful bibliography)
- X-rays of rectal bodies at the Berlin Charité
- Sturz in die Kiste. In: Der Spiegel Ausgabe 41, 1991, S. 317–320.
- Alles im A… In: einestages vom 7. Juni 2007