Polydactyly
Polydactyly or polydactylism (from Greek πολύς (polys), meaning 'many', and δάκτυλος (daktylos), meaning 'finger'),[1] also known as hyperdactyly, is a congenital physical anomaly in humans and animals resulting in supernumerary fingers and/or toes.[2] Polydactyly is the opposite of oligodactyly (fewer fingers or toes).
| Polydactyly | |
|---|---|
| Other names | Hyperdactyly |
 | |
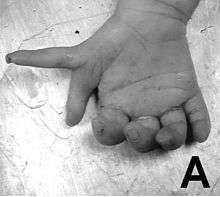
| Left hand with postaxial polydactyly | |
| Specialty | Medical genetics |
Signs and symptoms

In humans/animals this condition can present itself on one or both hands. The extra digit is usually a small piece of soft tissue that can be removed. Occasionally it contains bone without joints; rarely it may be a complete functioning digit. The extra digit is most common on the ulnar (little finger) side of the hand, less common on the radial (thumb) side, and very rarely within the middle three digits. These are respectively known as postaxial (little finger), preaxial (thumb), and central (ring, middle, index fingers) polydactyly. The extra digit is most commonly an abnormal fork in an existing digit, or it may rarely originate at the wrist as a normal digit does.[3]
The incidence of congenital deformities in newborns is approximately 2%, and 10% of these deformities involve the upper extremity.[4][5] Congenital anomalies of the limb can be classified in seven categories, proposed by Frantz and O’Rahilly and modified by Swanson, based on the embryonic failure causing the clinical presentation. These categories are failure of formation of parts, failure of differentiation, duplication, overgrowth, undergrowth, congenital constriction band syndrome, and generalized skeletal abnormalities.[6][7] Polydactyly belongs to the category of duplication.[8] Because there is an association between polydactyly and several syndromes, children with a congenital upper extremity deformity should be examined by a geneticist for other congenital anomalies. This should also be done if a syndrome is suspected, or if more than two or three generations of the family are affected.[9] Research has shown that the majority of congenital anomalies occur during the 4-week embryologic period of rapid limb development.[8] Polydactyly has been associated with 39 genetic mutations.[10] More specific loci and genetic mechanisms responsible for disorders of duplications will be defined with time, as molecular research continues.[8] Polydactyly can be divided into three major types, which are discussed below.
Ulnar or postaxial polydactyly
This is the most common situation, in which the extra digit is on the ulnar side of the hand, thus the side of the little finger. This can also be called postaxial polydactyly. It can manifest itself very subtly, for instance only as a nubbin on the ulnar side of the little finger, or very distinctly, as a fully developed finger. Most commonly, the extra finger is rudimentary, consisting of an end phalanx with a nail, and connected to the hand with a small skin pedicle. Mostly one neurovascular bundle can be identified, with no tendons present in the extra digit. In case of a fully developed extra finger, the duplication usually presents itself at the level of the metacarpophalangeal joint. A triplication of the little finger is very rare. Ulnar polydactyly occurs ten times more often in African populations.[11] The incidence in Caucasians is reported as 1 in 1,339 live births, compared with 1 in 143 live births in Africans and African Americans. Ulnar polydactyly is also often part of a syndrome.[11] In patients with African ancestry ulnar polydactyly mostly occurs isolated, whereas the presentation in Caucasians is often associated with a syndrome.[8] Though in a retrospective review, only 4 of 37 cases of ulnar polydactyly in Caucasians were syndromic.[12] In almost 14% of all patients, this type of polydactyly is hereditary. It usually passes on in an autosomal dominant manner with variable expression and incomplete penetrance. It is genetically heterogenic, meaning that mutations in different genes can be the cause. When the extra digit is pedicled it can be very movable; however, injuries are rare and have never been reported so far.
Radial or preaxial polydactyly
This is a less common situation, in which the affectation is on the side of the hand towards the thumb. Radial polydactyly refers to the presence of an extra digit (or extra digits) on the radial side of the hand. It is most frequent in Indian populations and it is the second most common congenital hand disorder. The incidence of radial polydactyly is reported as 1 in every 3,000 live births.[13] The clinical features of radial polydactyly will depend upon the extent of duplication.[11] Radial polydactyly varies from a barely visible radial skin tag to complete duplication. Thumb polydactyly varies from barely visible broadening of the distal phalanx to full duplication of the thumb including the first metacarpal.[14] Radial polydactyly is frequently associated with several syndromes.[15]
Central polydactyly
This is a very rare situation, in which the extra digit is on the ring, middle or index finger. Of these fingers, the index finger is most often affected, whereas the ring finger is rarely affected.[16] This type of polydactyly can be associated with syndactyly, cleft hand and several syndromes.[17][18] Polysyndactyly presents various degrees of syndactyly affecting fingers three and four.[14]
Causes
Polydactyly is associated with different mutations, either mutations in a gene itself or in a cis-regulatory element responsible for the expression of a specific gene. Mutations in Hoxa- or Hoxd clusters are reported leading to polydactyly. Interactions of Hoxd13 and GLI3 induce synpolydactyly, a combination of extra and consolidated digits. Other signal transduction pathways in this context are the Wnt signaling pathway or Notch.[19]
In the specific case of preaxial polydactyly (Hemingway mutant), a cis-acting mutation approximately 1Mb upstream of Shh gene has been implicated.[20] Normally Shh is expressed in an organiser region, called the zone of polarizing activity (ZPA) on the posterior limb side. From there it diffuses anteriorly, laterally to the growth direction of the limb. In the mutant, smaller ectopic expression in a new organiser region is seen on the anterior side of the limb. This ectopic expression causes cell proliferation delivering the raw material for one or more new digits.[20][21][22]
In addition to the study of genetic causes of polydactyly limb patterning models are used to simulate the congenital disorder at the limb, being able to explain the development paths of polydactyly.
Polydactyly can occur by itself, or more commonly, as one feature of a syndrome of congenital anomalies. When it occurs by itself, it is associated with autosomal dominant mutations in single genes, i.e. it is not a multifactorial trait.[23] But mutation in a variety of genes can give rise to polydactyly. Typically the mutated gene is involved in developmental patterning, and a syndrome of congenital anomalies results, of which polydactyly is one feature or two.
Types include:
| OMIM | Type | Locus |
|---|---|---|
| 174200 | Postaxial A1 | GLI3 at 7p13 |
| 602085 | Postaxial A2 | 13q21-q32 |
| 607324 | Postaxial A3 | 19p13.2-p13.1 |
| 608562 | Postaxial A4 | 7q22 |
| 174400 | Preaxial I | ? |
| 174500 | Preaxial II | SHH at 7q36 |
| 174600 | Preaxial III | ? |
| 174700 | Preaxial IV | GLI3 at 7p13 |
97 genetic syndromes have been associated with different kinds of polydactyly.[9]
Ulnar polydactyly
Ulnar polydactyly is often bilateral and associated with syndactyly and polydactyly of the feet. This can be a simple or complex polydactyly. Ulnar polydactyly occurs as an isolated congenital condition, but can also be part of a syndrome. The syndromes which occur with ulnar polydactyly are: Greig cephalopolysyndactyly syndrome, Meckel syndrome, Ellis–van Creveld syndrome, McKusick–Kaufman syndrome, Down syndrome, Bardet–Biedl syndrome, Smith–Lemli–Opitz syndrome[11][24]
Radial polydactyly
Type VII of radial polydactyly is associated with several syndromes: Holt–Oram syndrome, Fanconi anemia (aplastic anemia by the age of 6), Townes–Brocks syndrome, and Greig cephalopolysyndactyly (also known to occur with ulnar polydactyly).[15]
Central polydactyly
The syndromes associated with central polydactyly are: Bardet–Biedl syndrome,[25] Meckel syndrome,[26] Pallister–Hall syndrome,[27] Legius syndrome,[28] Holt–Oram syndrome,[29] Also, central polydactyly can be associated with syndactyly and cleft hand.[17][18]
Other syndromes including polydactyly include acrocallosal syndrome, basal cell nevus syndrome, Biemond syndrome, ectrodactyly-ectodermal dysplasias-cleft lip/palate syndrome, mirror hand deformity, Mohr syndrome, oral-facial-digital syndrome, Rubinstein-Taybi syndrome, short rib polydactyly, and VATER association.[30] It can also occur with a triphalangeal thumb.
Diagnosis


Classification is performed by using x-ray imaging to see the bone structures.[16]
Ulnar polydactyly

The classification of ulnar polydactyly exists of either two or three types. The two-stage classification, according to Temtamy and McKusick, involves type A and B. In type A there is an extra little finger at the metacarpophalangeal joint, or more proximal including the carpometacarpal joint. The little finger can be hypoplastic or fully developed. Type B varies from a nubbin to an extra, non-functional little finger part on a pedicle. According to the three-type classification, type I includes nubbins or floating little fingers, type II includes duplications at the MCPJ, and type III includes duplications of the entire ray.[31]
Radial polydactyly
The Wassel classification is the most widely used classification of radial polydactyly,[8] based upon the most proximal level of skeletal duplication. The most common type is Wassel 4 (about 50% of such duplications) followed by Wassel 2 (20%) and Wassel 6 (12%).[8]
Central polydactyly
The classification of central polydactyly is based on the extent of duplication and involves the following three types: Type I is a central duplication, not attached to the adjacent finger by osseous or ligamentous attachments; it frequently does not include bones, joints, cartilage, or tendons. Type IIA is a nonsyndactylous duplication of a digit or part of a digit with normal components, and articulates with a broad or bifid metacarpal or phalanx. Type IIB is a syndactylous duplication of a digit or part of a digit with normal components, and articulates with a broad or bifid metacarpal or phalanx. Type III is a complete digital duplication, which has a well-formed duplicated metacarpal.[17]
Treatment
Ulnar polydactyly
Ulnar polydactyly usually does not interfere with hand function, but for social reasons it can be treated operatively.[9]

Type A ulnar polydactyly
The treatment of Type A ulnar polydactyly is complex as its goal is to remove the accessory digit while maintaining a stable, functional small finger. When the duplicated proximal phalanx articulates with a common, broad metacarpal head, the ulnar collateral ligament must be considered. In those cases with a common articulation or with a sixth metacarpal the muscle executing the abduction of the little finger (abductor digiti minimi) must be preserved.[8] In patients with a common metacarpal articulation an elliptical incision at the base of the post-axial digit is made. This incision may be extended proximally in order to adequately expose the abductor digiti minimi. The ulnar collateral ligament and the insertions of the abductor digiti minimi are then elevated with a periosteal sleeve. The duplicated extensor and flexor tendons to the ulnar digit are transected and after that the digit is amputated at its articulation with the metacarpal. If the articular surface is wide the metacarpal may be shaved. At last the collateral ligament and abductor digiti minimi are reinserted at the base of the preserved proximal phalanx and a wire is then placed across the reconstructed joint. In patients with a duplicated metacarpal, the accessory digit is amputated in a standard ray fashion with transfer of the abductor digiti minimi to the retained small finger.[8]
Type B ulnar polydactyly
In this situation there is an absence of osseous and ligamentous structures. The surgical technique is analogous to radial polydactyly, in which the level of duplication and anatomical components should guide operative treatment.[8] The pedicled ulnar extra digit can be removed by suture ligation to devise the skin bridge of the newborn child. This might be easier than an excision of the extra digit when the child is 6 to 12 months old.[8][11] Ligation occludes the vascular supply to the duplicated digit, resulting in dry gangrene and subsequent autoamputation.[8] This must be done with consideration of the presence of a neurovascular bundle, even in very small skin bridges. When the ligation is done inappropriately it can give a residual nubbin. Also, a neuroma can develop in the area of the scar. An excision can prevent the development of a residual nubbin and the sensibility due to a neuroma.[11] For infants with ulnar type B polydactyly the recommended treatment is ligation in the neonatal nursery. Studies have shown that excision of the extra digit in the neonatal nursery is a safe and simple procedure with a good clinical and cosmetic outcome.[32]
Radial polydactyly
Because neither of the two thumb components is normal, a decision should be taken on combining which elements to create the best possible composite digit. Instead of amputating the most hypoplastic thumb, preservation of skin, nail, collateral ligaments and tendons is needed to augment the residual thumb.[33] Surgery is recommended in the first year of life, generally between 9 and 15 months of age.[8]
Surgical options depend on type of polydactyly.[34]
Bilhaut-Cloquet procedure
This type of procedure is recommended for Wassel types 1 and 2 (in which both thumbs are severely hypoplastic) by some congenital hand surgeons.[35] The technique contains a composite wedge resection of the central bone and soft-tissue. This will be achieved with approach of the lateral tissue of each thumb. The goal is to achieve a normal thumb, what concerns the size, which is possible.[8] If the width of the nail bed is greater than 70% of the contralateral thumb, it may be split.[36][37] Then the nail bed will be repaired precisely.
Ablation with collateral ligament reconstruction
This type of procedure is used for all Wassel types of polydactyly and is the most commonly used technique. It is recommended in all cases of thumb duplication with a hypoplastic, less-functional thumb. Otherwise, one could consider the Bilhaut-Cloquet. The ulnar thumb is preferably preserved as it is the more developed one in most cases.[8]
By detaching the radial collateral ligament from distal to proximal, a periosteal sleeve can be preserved.[38] In this way, the radial collateral band of the radial digit, will function as the absent radial collateral ligament of the preserved ulnar thumb.
Elevation of the APB and FPB is performed in Wassel type 4 duplication; this can be accomplished via the periosteum or separately. As the tendons insert proximally, the elevation is performed proximally too to potentially rebalance the ulnar thumb. After the radial thumb is amputated, the ulnar elements are centralized and fixed with a Kirschner wire. In most cases, a longitudinal and sagittal osteotomy is needed to centralize the bony parts of the ulnar thumb. While the soft-tissue of the radial thumb was preserved, it is now attached to the radial side of the ulnar thumb together with the periosteal sleeve. The APB and FPB of the ablated radial thumb are attached to the distal phalanx for more stability. If necessary, the extensor pollicis longus and the flexor pollicis longus are reattached to centralize their course.[8]
In Wassel type 5 and 6 the opponens pollicis muscle must be transferred to the ulnar metacarpal. Soft tissue with collateral ligament reconstruction is used to avoid any angular deformity in the preserved thumb. Tendon centralization is also often used for correction. Still, cases with osseous deformities may happen. To provide alignment, osteotomies are necessary to be done. This operation may need bone grafting, which is obtained from the amputated thumb.[8]
On top plasty procedure
This type is indicated when one thumb is larger proximally and the other thumb has a larger distal component. (The procedure is initially described as a way to lengthen amputated digits.) The goal is to create a functional thumb by combining less-hypoplastic components. On top plasty procedure is rarely employed in the treatment of congenital thumb duplication. It might be necessary for Wassel types 4, 5, 6.[8]
At the level of the mid-proximal phalanx or mid-metacarpal, the distal component is transferred to the proximal component. The tendons of the distal component are preserved as the rest of the distal component is amputated. The neurovascular bundle which supplies the distal component is reserved and transferred proximally.[8]
Central polydactyly
Early osteotomy and ligament reconstructions should be done to prevent deformities, such as angular growth deformities.[15]
The surgical treatment of central polydactyly is highly variable. After the surgery the hand must be functional and stable, but also aesthetically pleasing. This requires intraoperative creativity and flexibility. The surgeon must also consider whether retention of a fully functional supranumerary digit is preferable to surgical intervention. In contrast, a functional, four-fingered hand achieved via ray amputation may be preferable to a five-fingered hand with a deformed or stiff reconstructed finger.[8]
Cases of polysyndactyly are approached through a standard opposing zig-zag incision. The incision is favored toward the accessory digit, preserving extra skin for subsequent closure. Depending on the level and extent of duplication, the flexor and extensor tendons may require centralization or rebalancing. Also, the collateral ligaments must be preserved or reconstructed. Wide articular surfaces should be narrowed and phalangeal wedge osteotomies may be required to provide an axial alignment. Attention must also be given to reconstruct the intermetacarpal ligament. Furthermore, one should take in mind the provision for adequate web-space soft tissue.[8]
Prognosis
Ulnar polydactyly
Type A ulnar polydactyly
There are no substantive outcome studies regarding the function of these hands following surgical intervention. This is mainly caused by the fact that there is a generally normal function of these patients’ hands following ablation with collateral ligament reconstruction.[8] In a study on 27 patients undergoing surgical excision for Type A ulnar polydactyly, only one complication was noted in the form of an infection[39] However, no investigators have objectively reviewed functional range of motion or articular stability.[8]
Type B ulnar polydactyly
In a study on 21 patients with Type B ulnar polydactyly treated with suture ligation it was found that the duplicated digit was typically amputated at an average of 10 days and no complications of infection or bleeding were reported.[40] In a large study on 105 patients treated with suture ligation an overall complication rate of 23.5% was reported, citing a residual tender or unacceptable bump in 16%, infection in 6%, and bleeding in 1% of patients.[39] In general, suture ligation is safe and effective when applied to appropriate cases of Type B polydactyly in which no substantial ligamentous or osseous structures are present within the pedicle. Parents should be educated as to the progression of necrosis, and that revision of residual tissue or scar may be necessary when the child is 6 months of age or older.[8]
Radial polydactyly
Bilhaut procedure
Advantages: By combining two hypoplastic thumbs a sufficient thumb size is acquired. Furthermore, the IP and MCP joints are very stable as the collateral ligaments are not violated during reconstruction.[8] Disadvantages: Violation during reconstruction can lead to growth arrest or asymmetric growth. Nail deformity could also occur after reconstruction. Although the joints are stable, restriction of flexion may be possible.[8] The average IP flexion in a reconstructed thumb is 55 degrees less than the contralateral thumb. MCP flexion averaged 55 degrees in reconstructed thumbs, compared to 75 degrees in the contralateral thumb.[34]
Ablation with collateral ligament reconstruction
Advantages: The reconstructed joints tend to remain flexible. Also, it preserves the nail bed and physis, this increases the prevention of nail deformities over time.[8] Disadvantages: Although surgeons try to obtain a stable thumb of appropriate size, instability of the IP and MCP joint may occur, as well as a size mismatch. Thumbs are defined as unacceptable if IP joint deviation exceeds 15 degrees, MCP joint deviation exceeds 30 degrees, and thumb size is inappropriate based on the examiner’s assessment. Also, thumb size one-third greater or less than the contralateral thumb is defined as unacceptable.[8]
On-top plasty procedure
No surgical outcomes studies exist for evaluating the function of the thumbs after an on-top plasty reconstruction.[8]
Central polydactyly
Few clinical outcome studies exist regarding the treatment of central polydactyly. Tada and colleagues note that satisfactory surgical correction of central polydactyly is difficult to achieve and that outcomes are generally poor. In Tada’s study, 12 patients were reviewed. All patients required secondary surgical procedures to address flexion contractures and angular deviation at the IP joint level.[18] However, several primary factors contribute to the complexity of central polydactyly reconstruction. Hypoplastic joints and soft tissues that predispose the reconstructed finger to joint contracture, and angular deformities as well as complex tendon anomalies, are often difficult to address. Therefore, treatment is wholly dependent on the anatomic components present, the degree of syndactyly, and the function of the duplicated finger.[18]
Epidemiology
The condition has an incidence of 1 in every 500 live births. Postaxial hand polydactyly is a common isolated disorder in African black children, and autosomal dominant transmission is suspected. Postaxial polydactyly is more frequent in native Africans living in the Eastern and Central than the Caucasians and Mongoloids and is more frequent in male children.[41] In contrast, postaxial polydactyly seen in white children is usually syndromic and associated with an autosomal recessive transmission. One study by Finley et al. combined data from Jefferson County, Alabama, United States, and Uppsala County, Sweden. This study showed incidence of all types of polydactyly to be 2.3 per 1000 in Caucasian males, 0.6 per 1000 in Caucasian females, 13.5 per 1000 in African males, and 11.1 per 1000 in African females.[30]
Society and culture
.jpg)
People with polydactyly
- A boy named Hong Hong born in Pingjiang County, Hunan province, China, in January 2016 has 31 fingers and toes.[42][43]
- Akshat Saxena from Uttar Pradesh, India, is the world record holder for highest number of digits. He was born in 2010 with 7 digits on each hand and 10 digits on each foot, for a total of 34 digits.[44]
- Zerah Colburn, American prodigious math calculating savant.[45]
- Anne Boleyn, former Queen of England, was rumoured to have six fingers on one hand. However, considering that this rumour first emerged in the 1580s from a Catholic dissenter, it is generally deemed false.[46]
- Antonio Alfonseca, professional baseball player known as "El Pulpo" - Spanish for "the Octopus" with regard to his extra digit on each extremity
- Hampton Hawes, jazz pianist, was born with six fingers on each hand (the extra fingers were surgically removed shortly after birth).[47]
- Henry II the Pious, High Duke of Poland 1238–1241, had six toes on his left foot.[48]
- Lucille Clifton, an African-American poet and civil rights advocate
- Robert Chambers, purported author of Vestiges of the Natural History of Creation, and his brother William: six digits each limb
- Kamani Hubbard, a boy born with a rare case of polydactyly, with 12 fingers and 12 toes all fully functional[49]
- Varalakshmi V, a girl from Bangalore with eight fingers in each hand and about four to five extra toes in each foot[50]
- David Laksono, a Chinese-Indonesian professional interior designer and fashion model – born with a supernumerary thumb on his left hand
- Hrithik Roshan, a Bollywood actor born with a supernumerary thumb on his right hand
- Nayanthara, an Indian actress, with a rudimentary finger on her left hand
- Garfield Sobers, West Indian cricketer, had an extra finger on each hand which he removed himself during childhood "with the aid of catgut and a sharp knife"[51]
- Danny Garcia, boxing champion, has 6 toes on his right foot.
- Mao Tse-tung's third wife Jiang Qing reportedly had six toes on her right foot.[52]
- Drew Carey, actor and comedian, has six toes on his right foot, according to his autobiography.
- Yoandri Hernández Garrido, nicknamed "Veinticuatro" ("twenty four" in Spanish), has six fully formed fingers on both hands and six perfect toes on each foot.[53]
- American Chicago blues guitarist Hound Dog Taylor was born with polydactyly on both hands, although around age 41, he removed the extra finger on his right hand.[54]
- Volcacius Sedigitus, a Roman poet of the 1st century, probably received his epithet, signifying "Sixfinger", because he was born with six fingers on each hand, according to Pliny,[55]
- Lower Styrian baron Johann Jacob Freiherr von Moscon (1621-1661) is depicted with six fingers at his left hand on a portrait from Brežice, Slovenia.
- Zachariah Dean, Master of the Procedure Civilly.[55]
- Marycarol Park, attorney and child welfare activist, was born with six toes on her right foot.
- Many members of the Da Silva family in Sao Paulo family in Brazil have 6 fingers on each hand.[56]
- Brites de Almeida, a semi-legendary Portuguese woman who killed seven hiding Castilian soldiers in her oven after the Battle of Aljubarrota, had six fingers on each hand.
- Arpit Buchha from Bikaner Rajasthan has 6 fingers in his left hand.
- Zhu Yunming, a Chinese calligrapher, had 6 fingers in his right hand.
- Fictional serial killer Hannibal Lecter is described in the Thomas Harris novel The Silence of the Lambs as having a left hand with mid ray duplication polydactyly, i.e. a duplicated middle finger.[57]
- The actress Gemma Arterton was born with six fingers on each hand, the extra fingers removed after birth.
Other animals
Polydactyly occurs in numerous types of animals. The defect is sporadically seen in livestock, where it affects cattle, sheep, pigs, and occasionally horses.[58] Conversely, it is a common trait in several heritage chicken breeds. Chickens normally have 4 toes on each foot. The chicken breeds known for being polydactyl are the Dorking, Faverolle, Houdan, Lincolnshire Buff, Meusienne, Sultan, and non-bearded Silkie Bantams.[59][60] The breed standard of these varieties of chickens calls for 5 toes on each foot, although sometimes more than 5 toes will occur. The extra digit in these breeds presents as an extra "thumb" that does not touch the ground.[59] Mixed-breed chickens may also have extra digits if the aforementioned breeds are part of their genetic makeup.
Polydactyly also occurs in dogs, cats, and small mammals such as guinea pigs[61] and mice. [62] Cats normally have five digits on the front paws and four on the rear. Polydactyl cats have more, and this is a moderately common condition, especially in certain cat populations. Dogs, like other canids, normally have four claws on their rear paws; a fifth is often called a dewclaw and is especially found in certain dog breeds,[63] including the Norwegian Lundehund and Great Pyrenees.
A number of mutations of the LMBR1 gene, in dogs, humans, and mice, can cause polydactyly.[63] A 2014 report indicated that mice could also exhibit polydactyly arising from mutation in the VPS25 gene.[64] In cattle, it appears to be polygenic with a dominant gene at one locus and a homozygous recessive at another.[58]
Polydactyly was believed to be common in early tetrapods, the extinct amphibians that represented the earliest landliving vertebrates. Their number of toes fluctuated until the early Carboniferous period when they finally began developing a uniform number of toes. Amniotes settled on five toes per limb, while amphibians developed four toes on each front limb and five toes on each back limb. (For more information, see Polydactyly in early tetrapods). Polydactyly also occurs in modern extant reptiles[65] and amphibians.[66]
 Rooster with feathered legs (Aldrovandi himself did not notice the five toes)[67]
Rooster with feathered legs (Aldrovandi himself did not notice the five toes)[67] Kitten with 23 toes
Kitten with 23 toes Muscovy duck, both feet have 5 toes
Muscovy duck, both feet have 5 toes Muscovy duck, both feet have 5 toes
Muscovy duck, both feet have 5 toes
References
- "Polydactyly Etymology". Online Etymology Dictionary. Retrieved February 13, 2016.
- Kaneshiro, Neil K. "Polydactyly - Overview". University of Maryland Medical Center (UMMC). Retrieved 5 January 2013.
- Eaton, Charles. "Polydactyly (Extra Fingers)". Retrieved 9 February 2010.
- Flatt AE (1977). The care of congenital hand anomalies. St. Louis: Mosby.
- McCarroll HR (2000). "Hand anomalies". J Hand Surg [Am]. 25 (6): 1007–37. doi:10.1053/jhsu.2000.6457. PMID 11119659.
- Frantz CH; O’Rahilly R (1961). "Congenital skeletal limb deficiencies". J Bone Joint Surg Am. 43 (8): 1202–24. doi:10.2106/00004623-196143080-00012.
- Swanson AB (1976). "A classification for congenital limb malformations". J Hand Surg Am. 1 (1): 8–22. doi:10.1016/s0363-5023(76)80021-4. PMID 1021591.
- Watt AJ, Chung KC (2009). "Duplication". Hand Clin. 25 (2): 215–227. doi:10.1016/j.hcl.2009.01.001. PMID 19380061.
- Van Nieuwenhoven C, Boehmer A, Hovius S (2009). "Polydactyly". Praktische Pediatrie. 2.
- Biesecker LG (2002). "Polydactyly: how many disorders and how many genes". Am J Med Genet. 12 (3): 279–83. doi:10.1002/ajmg.10779. PMID 12357471.
- Buck-Gramcko D (1998). Congenital malformations of the hand and forearm. Churchill-Livingstone.
- Reyen, GM (2001). "Ulnar polydactyly". Plastic and Reconstructive Surgery. 107 (6): 1449–54, discussion 1455–7. doi:10.1097/00006534-200105000-00021. PMID 11335816.
- Jobe MT (2008). Congenital anomalies of the hand. Canale ST, Beaty JH, Editors. Campbell's Operative Orthopaedics. 11. pp. 4367–449. doi:10.1016/b978-0-323-03329-9.50079-9. ISBN 9780323033299.
- wikibooks. Handbook of genetic counseling/polydactyly and syndactyly.
- "Summary of most common syndromes with concomitant polydactyly".
- "Pictures of Extra Fingers" (in Dutch). Archived from the original on 11 November 2013.
- Graham TJ, Ress AM (1998). "Finger polydactyly". Hand Clin. 14 (1): 49–64. PMID 9526156.
- Tada K, Kurisaki E, Yonenobu K, et al. (1982). "Central polydactyly- a review of 12 cases and their surgical treatment". J Hand Surg [Am]. 7 (5): 460–5. doi:10.1016/s0363-5023(82)80040-3. PMID 7130654.
- Lange, Axel, Nemeschkal, Hans L., Müller, Gerd B.. Evolutionary Biology, Dec. 2013
- Lettice LA, Heaney SJ, Purdie LA, Li L, de Beer P, Oostra BA, Goode D, Elgar G, Hill RE, de Graaff E (2003). "A long-range Shh enhancer regulates expression in the developing limb and fin and is associated with preaxial polydactyly" (PDF). Human Molecular Genetics. 12 (14): 1725–35. doi:10.1093/hmg/ddg180. PMID 12837695.
- Lettice LA, Hill AE, Devenney PS, Hill RE (2008). "Point mutations in a distant sonic hedgehog cis-regulator generate a variable regulatory output responsible for preaxial polydactyly". Human Molecular Genetics. 17 (7): 978–85. doi:10.1093/hmg/ddm370. PMID 18156157.
- Lettice LA, Williamson I, Wiltshire JH, Peluso S, Devenney PS, Hill AE, Essafi A, Hagman J, Mort R, Grimes G, DeAngelis CL, Hill RE (2012). "Opposing functions of the ETS factor family define Shh spatial expression in limb buds and underlie polydactyly". Developmental Cell. 22 (2): 459–67. doi:10.1016/j.devcel.2011.12.010. PMC 3314984. PMID 22340503.
- "Polydactyly and Syndactyly". Milton S. Hershey Medical Center. Archived from the original on 2010-03-07. Retrieved 9 February 2010.
- Nicolai JP, Hamel BC, Menalda GA (1990). "[Polydactyly]". Nederlands Tijdschrift voor Geneeskunde (in Dutch). 134 (4): 157–9. PMID 2304571.
- Kumar S, Mahajan BB, Mittal J (2012). "Bardet-Biedl syndrome: a rare case report from North India". Indian J Dermatol Venereol Leprol. 78 (9): 228. doi:10.4103/0378-6323.93656. PMID 22421669.
- Panduranga C, Kangle R, Badami R, Patil PV (2012). "Meckel-Gruber syndrome: Report of two cases". J Neurosci Rural Pract. 3 (1): 56–9. doi:10.4103/0976-3147.91943. PMC 3271618. PMID 22346195.
- Biesecker LG (1993). Pallister-Hall Syndrome.
- Denayer E, Chmara M (2011). "Legius syndrome in fourteen families". Hum. Mutat. 32 (1): 1985–98. doi:10.1002/humu.21404. PMC 3038325. PMID 21089071.
- Fryns JP, Bonnet D, De Smet L (1996). "Holt-Oram syndrome with associated postaxial and central polydactyly. Further evidence for genetic heterogeneity in the Holt-Oram syndrome". Genet Couns. 7 (4): 323–4. PMID 8985738.
- Supernumerary Digit at eMedicine
- Temtamy SA, McKusick VA (1978). "The genetics of hand malformations". Birth Defects Orig Artic Ser. 14 (3): 1–619.
- Katz K, Linder N (2011). "Postaxial type B polydactyly treated by excision in the neonatal nursery". J Pediatr Orthop. 31 (4): 448–9. doi:10.1097/bpo.0b013e31821addb6. PMID 21572283.
- Light TR (1992). "Treatment of preaxial polydactyly". Hand Clin. 8 (1): 161–75. PMID 1572920.
- Tonkin MA, Bulstrode NW (2007). "Bilhaut-Cloquet procedure for Wassel types III, IV and VII thumb duplication". J Hand Surg Eur. 32 (6): 684–93. doi:10.1016/j.jhse.2007.05.021. PMID 17993432.
- Bilhaut M. (1889). "Guerison d'un pouce bifide par un nouveau procede operatoire". Conges Francais de Chirurgie. 4: 576–80.
- Tada K, Yonenobu K, Tsuyuguchi Y, et al. (1983). "Duplication of the thumb: a retrospective review of two hundred and thirty seven cases". J Bone Joint Surg Am. 65 (5): 584–98. doi:10.2106/00004623-198365050-00002. PMID 6853563.
- Dobyns JH, Lipscomb PR, Cooney WP (1985). "Management of thumb duplication". Clin Orthop Relat Res. 195: 26–44.
- Manske PR (1989). "Treatment of duplicated thumb using a ligamentous/periosteal flap". J Hand Surg [Am]. 14 (4): 728–33. doi:10.1016/0363-5023(89)90200-1. PMID 2754208.
- Rayan GM, Frey B (2001). "Ulnar polydactyly". Plast Reconstr Surg. 107 (6): 1449–54. doi:10.1097/00006534-200105000-00021. PMID 11335816.
- Watson BT, Hennrikus WL (1997). "Postaxial type-B polydactyly". J Bone Joint Surg Am. 79 (1): 65–8. doi:10.2106/00004623-199701000-00007. PMID 9010187.
- Kaneshiro, Neil K.; David Zieve (11 February 2009). "Polydactyly". Penn Medicine. Retrieved 9 February 2010.
- "Chinese boy born with 31 fingers and toes".
- "Chinese Baby Born with 31 Fingers and Toes". 2016-05-05.
- David W. Freeman (July 25, 2011). "Akshat Saxena sets Guinness record for most fingers, toes". CBS News. Retrieved February 13, 2016.
- Colburn, Zerah (1833). "A Memoir of Zerah Colburn".
- Bordo, Susan (2013). The Creation of Anne Boleyn: A New Look at England's Most Notorious Queen. New York: Houghton Mifflin Harcourt. page 23. ISBN 978-0547328188.
- Harrison, Dennis. "Hamptom Hawes And The Fire Inside". JazzScript. Retrieved 9 February 2010.
- Historyczne, Polskie Towarzystwo (1961). Mowia, wieki: magazyn historyczny (in Polish). Państwowe Zakłady Wydawn. Szkolnych. p. 52.
- Baby in California born with 12 functioning fingers and toes, in a rare case of polydactylism
- (http://www.ndtv.com/article/cities/hope-for-bangalore-girl-with-27-fingers-and-toes-49433?pfrom=Cities&cp
- Sobers, Garfield (1 May 2002). Garry Sobers: My Autobiography. Headline Book Publishing. p. 6. ISBN 978-0-7553-1006-7.
- Li, Zhisui (1994). The Private Life of Chairman Mao. Random House. ISBN 978-0-679-76443-4.
- "Interview Exclusive - Yoandri Hernandez Garrido - 24 fingers". Cubastyletv. Retrieved 18 January 2013.
- "Hound Dog Taylor – Everyone Knows the Hound". TheDeltaBlues. Archived from the original on 2013-11-06.
- nh ii.214.
- "There's something a bit different about this family from Brazil". 2015-09-16.
- Harris, Thomas (1988). Silence of the Lambs. New York City: St. Martin's Press. p. 15.
Dr. Lecter has six fingers on his left hand
- Hanson, DMV, Russell. "Congenital and Inherited Anomalies of the Musculoskeletal System in Multiple Species". Merck Sharp & Dohme Corp. Retrieved 8 April 2018.
- "Chicken Feet". University of Illinois Extension: Incubation and Embryology. University of Illinois Board of Trustees. Retrieved 4 April 2017.
- Elio, C; Moiseyeva, I; Romanov, M. (2010). "Five-Toed Chickens" (PDF). summagallicana.it. Izvestiya of ТАА. Retrieved 13 April 2017.
- Kazmeyer, Milton. "Polydactyly in Guinea Pigs". Whalerock Digital Media, LLC. Retrieved 8 April 2018.
- Fisher, R.A. (11 March 1950). "Polydactyly in Mice". Nature: International Journal of Science. Macmillan Publishers Limited. Retrieved 8 April 2018.
- Park, K; Kang, J; Subedi, Kp; Ha, Jh; Park, C (Aug 2008). "Canine Polydactyl Mutations With Heterogeneous Origin in the Conserved Intronic Sequence of LMBR1" (Free full text). Genetics. 179 (4): 2163–72. doi:10.1534/genetics.108.087114. ISSN 0016-6731. PMC 2516088. PMID 18689889.
- Handschuh, Karen; Feenstra, Jennifer; Koss, Matthew; et al. (23 October 2014). "ESCRT-II/Vps25 Constrains Digit Number by Endosome-Mediated Selective Modulation of FGF-SHH Signaling". Cell Reports. 9 (2): 674–87. doi:10.1016/j.celrep.2014.09.019. PMC 4223648. PMID 25373905. Lay summary – NIH Press Release (21 November 2014).
- Bauer, Aaron (24 December 2009). "Polydactyly in the Central Pacific Gecko" (PDF). Allen Press. Retrieved 8 April 2018.
- Cooper, John E. (25 April 1958). "Some Albino Reptiles and Polydactylous Frogs". Herpetologica. 14 (1): 54–56. JSTOR 3890281.
- Ornithologiae, Ulisse Aldrovandi (ill. Cristoforo Coriolano), 1599