Nasopharyngeal angiofibroma
Nasopharyngeal angiofibroma is a histologically benign but locally aggressive vascular tumor of the nasopharynx that arises from the superior margin of the sphenopalatine foramen and grows in the back of the nasal cavity. It most commonly affects adolescent males (because it is a hormone-sensitive tumor). Though it is a benign tumor, it is locally invasive and can invade the nose, cheek, orbit (frog face deformity), or brain.[3] Patients with nasopharyngeal angiofibroma usually present with one-sided nasal obstruction with profuse epistaxis.
| Nasopharyngeal angiofibroma | |
|---|---|
| Other names | Juvenile nasopharyngeal angiofibroma[1][2] |
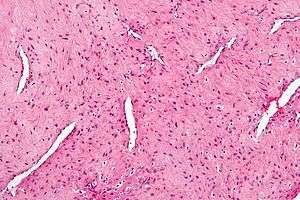 | |
| Micrograph of a nasopharyngeal angiofibroma H&E stain. | |
| Specialty | ENT surgery |
Signs and symptoms
- Frequent chronic epistaxis or blood-tinged nasal discharge
- Nasal obstruction and rhinorrhea
- Facial dysmorphism (when locally invasive)
- Conductive hearing loss from eustachian-tube obstruction
- Diplopia, which occurs secondary to erosion into superior orbital fissure and due to third and sixth nerve palsy.
- Proptosis when having intraorbital extension.
- Rarely anosmia, recurrent otitis media, and eye pain.
Diagnosis
If nasopharyngeal angiofibroma is suspected based on physical examination (a smooth vascular submucosal mass in the posterior nasal cavity of an adolescent male), imaging studies such as CT or MRI should be performed. Biopsy should be avoided as to avoid extensive bleeding since the tumor is composed of blood vessels without a muscular coat.
Antral sign or Holman-Miller sign (forward bowing of posterior wall of maxilla) is pathognomic of angiofibroma.
DSA (digital subtraction angiography) of carotid artery to see the extension of tumors and feeding vessels
Differential diagnosis
- Antro-choanal polyp (benign non neoplastic growth)[4]
- Rhinosporidiosis (as bleeding point is here too)
- Malignancy—nasopharyngeal carcinoma, lymphoma, plasmacytoma, rhabdomyosarcoma
- Chordoma
- Nasopharyngeal cyst
- Pyogenic granuloma
Treatment
Treatment for Nasopharyngeal angiofibroma (JNA) is primarily surgical. The tumor is primarily excised by external or endoscopic approach. Medical treatment and radiation therapy are only of historical interest.
External approaches:
- transpalatine approach
- transpalatine + sublabial (Sardana's) Approach
- infratemporal Approach
- nasal endoscopic Approach
- transmaxillary Approach
- maxillary swing Approach or Facial translocation
Endoscopic approach is an excellent tool in primary and recurrent JNA, it allows visualisation and precise removal of the lesion. Preoperative embolisation of tumour may be of some use in reducing intraoperative bleeding.(Mostly we do preoperative embolisation of maxillary artery. )
Direct visualization is not common.
- If the tumor is limited to nasopharynx and nose, for endoscopic approach or Wilson's transpalatal approach is used. It can be extended into Sardana's approach if the tumor extends laterally.
- For tumors of infratemporal fossa, Maxillary Swing approach is used.
- Transmaxillary Le Fort 1 approach is used for tumors extending into maxillary and ethmoid sinuses and pterygopalatine fossa.
- If the tumor extend up to the cheek, for Weber–Ferguson approach should be used.
Prognosis
Prognosis for nasopharyngeal angiofibroma is favorable. Because these tumors are benign, metastasis to distal sites does not occur. However, these tumors are highly vascularized and grow rapidly. Removal is important in preventing nasal obstruction and recurrent epistaxis. Mortality is not associated with nasopharyngeal angiofibroma.[5]
References
- 00021 at CHORUS
- "juvenile nasopharyngeal angiofibroma" at Dorland's Medical Dictionary
- Raphael Rubin; David S. Strayer; Emanuel Rubin (2008). Rubin's Pathology: clinicopathologic foundations of medicine. Lippincott Williams & Wilkins. pp. 1071–. ISBN 978-0-7817-9516-6. Retrieved 29 June 2010.
- Tos, Mirko; Larsen, Per L.; Larsen, Knud; Cayé-Thomasen, Per (2000), Stamm, Aldo Cassol; Draf, Wolfgang (eds.), "Nasal Polyps", Micro-endoscopic Surgery of the Paranasal Sinuses and the Skull Base, Springer Berlin Heidelberg, pp. 103–125, doi:10.1007/978-3-642-57153-4_8, ISBN 9783642571534, retrieved 2019-10-02
- Textbook of Family Medicine, 8th Edition. Chapter 19 p.329. Rakel, MD. ISBN 978-1-4377-1160-8
External links
| Classification | |
|---|---|
| External resources |