Management of Parkinson's disease
Management of Parkinson's disease due to the chronic nature of Parkinson's disease (PD), a broad-based program is needed that includes patient and family education, support-group services, general wellness maintenance, exercise, and nutrition. At present, no cure for the disease is known, but medications or surgery can provide relief from the symptoms.
| Management of Parkinson's disease | |
|---|---|
| Specialty | neurology |
While many medications treat Parkinson's, none actually reverses the effects of the disease. Furthermore, the gold-standard treatment varies with the disease state. People with Parkinson's, therefore, often must take a variety of medications to manage the disease's symptoms.[1] Several medications currently in development seek to better address motor fluctuations and nonmotor symptoms of PD. However, none is yet on the market with specific approval to treat Parkinson's.[2]
Medication
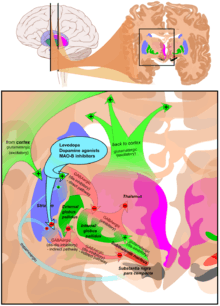
The main families of drugs useful for treating motor symptoms are Levodopa, dopamine agonists, and MAO-B inhibitors.[3] The most commonly used treatment approach varies depending on the disease stage. Two phases are usually distinguished: an initial phase in which the individual with PD has already developed some disability for which he or she needs pharmacological treatment, and a second stage in which the patient develops motor complications related to levodopa usage.[3] Treatment in the initial state aims to attain an optimal tradeoff between good management of symptoms and side effects resulting from enhancement of dopaminergic function. The start of L-DOPA treatment may be delayed by using other medications such as MAO-B inhibitors and dopamine agonists, in the hope of causing the onset of dyskinesias to be retarded.[3] In the second stage, the aim is to reduce symptoms while controlling fluctuations of the response to medication. Sudden withdrawals from medication, and overuse by some patients, also must be controlled.[3] When medications are not enough to control symptoms, surgical techniques such as deep brain stimulation can relieve the associated movement disorders.[4]
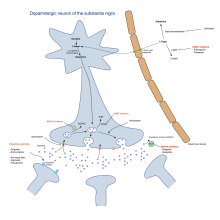
Levodopa

Levodopa (or L-DOPA) has been the most widely used treatment for over 30 years.[3] L-DOPA is transformed into dopamine in the dopaminergic neurons by dopa-decarboxylase.[3] Since motor symptoms are produced by a lack of dopamine in the substantia nigra, the administration of L-DOPA temporarily diminishes the motor symptomatology.[3]
Only 5–10% of L-DOPA crosses the blood–brain barrier. The remainder is often metabolised to dopamine elsewhere, causing a wide variety of side effects including nausea, dyskinesias, and stiffness.[3] Carbidopa and benserazide are peripheral dopa decarboxylase inhibitors.[3] They inhibit the metabolism of L-DOPA in the periphery, thereby increasing levodopa delivery to the central nervous system. They are generally given as combination preparations with levodopa.[3] Existing preparations are carbidopa/levodopa (co-careldopa, trade names Sinemet, Pharmacopa, Atamet) and benserazide/levodopa (co-beneldopa, trade name Madopar). Levodopa has also been related to a dopamine dysregulation syndrome, which is a compulsive overuse of the medication, and punding.[5]
Controlled, slow-release versions of Sinemet and Madopar spread out the effect of the levodopa. Duodopa is a combination of levodopa and carbidopa. Slow-release levodopa preparations have not shown an increased control of motor symptoms or motor complications when compared to immediate-release preparations.[3]
Tolcapone inhibits the catechol-O-methyltransferase (COMT) enzyme, which degrades dopamine and levadopa, thereby prolonging the therapeutic effects of levodopa.[3] It, alongside inhibitors of peripheral dopa decarboxylase, have been used to complement levodopa. However, due to its possible side effects such as liver failure, it is limited in its availability.[3] A similar drug, entacapone, has not been shown to cause significant alterations of liver function and maintains adequate inhibition of COMT over time.[3] Entacapone is available for treatment alone (COMTan) or combined with carbidopa and levodopa (Stalevo).[3]
Levodopa results in a reduction in the endogenous formation of L-DOPA, and eventually becomes counterproductive. Levodopa preparations lead in the long term to the development of motor complications characterized by involuntary movements called dyskinesias and fluctuations in the response to medication.[3] When this occurs, PD patients change rapidly from stages with good response to medication and few symptoms ("on" state) to phases with no response to medication and important motor symptoms ("off" state).[3] For this reason, levodopa doses are kept as low as possible while maintaining functionality.[3] Delaying the initiation of dopatherapy, using instead alternatives for some time, is also common practice.[3] A former strategy to reduce motor complications was to withdraw patients from L-DOPA for some time. It is discouraged now since it can bring dangerous side effects such as neuroleptic malignant syndrome.[3] Most people eventually need levodopa and later develop motor complications.[3]
The on-off phenomenon is an almost invariable consequence of sustained levodopa treatment in patients with Parkinson's disease. Phases of immobility and incapacity associated with depression alternate with jubilant thaws. Both pharmacokinetic and pharmacodynamic factors are involved in its pathogenesis, but evidence is presented to indicate the importance of levodopa handling has been underestimated and progressive reduction in the storage capacity of surviving nigrostriatal dopamine terminals is not a critical factor. Redistribution of levodopa dosage which may mean smaller, more frequent doses, or larger less frequent increments, may be helpful in controlling oscillations in some patients. Dietary protein restriction and the use of selegiline hydrochloride and bromocriptine may also temporarily improve motor fluctuations. New approaches to management include the use of subcutaneous apomorphine, controlled-release preparations of levodopa with a peripheral dopa decarboxylase inhibitor and the continuous intraduodenal administration of levodopa.
In animal models it was shown that the intake of Adenosine receptor antagonists together with Levodopa can amplify its therapeutic effects.[6][7]
Dopamine agonists
Dopamine agonists in the brain have a similar effect to levodopa since they bind to dopaminergic postsynaptic receptors.[3] Dopamine agonists were initially used for patients experiencing on-off fluctuations and dyskinesias as a complementary therapy to levodopa, but they are now mainly used on their own as an initial therapy for motor symptoms with the aim of delaying motor complications.[3][8] When used in late PD, they are useful at reducing the off periods.[3] Dopamine agonists include bromocriptine, pergolide, pramipexole, ropinirole, piribedil, cabergoline, apomorphine, and lisuride.
Agonists produce significant, although mild, side effects including somnolence, hallucinations, insomnia, nausea, and constipation.[3] Sometimes, side effects appear even at the minimal clinically efficacious dose, leading the physician to search for a different agonist or kind of drug.[3] When compared with levodopa, while they delay motor complications, they control worse symptoms.[3] Nevertheless, they are usually effective enough to manage symptoms in the initial years.[9] They are also more expensive.[9] Dyskinesias with dopamine agonists are rare in younger patients, but along other side effects, more common in older patients.[9] All this has led to agonists being the preferential initial treatment for the former as opposed to levodopa in the latter.[9] Agonists at higher doses have also been related to a wide variety of impulse-control disorders.[5]
Apomorphine, which is a dopamine agonist not orally administered, may be used to reduce off periods and dyskinesia in late PD.[3] Since secondary effects such as confusion and hallucinations are not rare, patients under apomorphine treatment should be closely monitored.[3] Apomorphine can be administered by subcutaneous injection using a small pump which is carried by the patient. A low dose is automatically administered throughout the day, reducing the fluctuations of motor symptoms by providing a steady dose of dopaminergic stimulation. After an initial "apomorphine challenge" in hospital to test its effectiveness and brief patient and primary caregiver (often a spouse or partner), the latter of whom takes over maintenance of the pump. The injection site must be changed daily and rotated around the body to avoid the formation of nodules. Apomorphine is also available in a more acute dose as an autoinjector pen for emergency doses such as after a fall or first thing in the morning. Nausea and vomiting are common, and may require domperidone (an antiemetic).
In a study evaluating the efficacy of dopamine agonists compared to levodopa, the results showed patients who took dopamine agonists were less likely to develop dyskinesia, dystonia, and motor fluctuations, although were more likely to discontinue therapy due to negative side effects such as nausea, edema, constipation, etc.
MAO-B inhibitors
Monoamine oxidase inhibitors (selegiline and rasagiline) increase the level of dopamine in the basal ganglia by blocking its metabolization. They inhibit monoamine oxidase-B (MAO-B) which breaks down dopamine secreted by the dopaminergic neurons. Therefore, reducing MAO-B results in higher quantities of L-DOPA in the striatum.[3] Similarly to dopamine agonists, MAO-B inhibitors improve motor symptoms and delay the need of taking levodopa when used as monotherapy in the first stages of the disease, but produce more adverse effects and are less effective than levodopa. Evidence on their efficacy in the advanced stage is reduced, although it points towards them being useful to reduce fluctuations between on and off periods.[3] Although an initial study indicated selegiline in combination with levodopa increased the risk of death, this has been later disproven.[3]
Metabolites of selegiline include L-amphetamine and L-methamphetamine (not to be confused with the more potent dextrorotary isomers). This might result in side effects such as insomnia. Another side effect of the combination can be stomatitis. Unlike other nonselective monoamine oxidase inhibitors, tyramine-containing foods do not cause a hypertensive crisis.
Other drugs
Some evidence indicates other drugs such as amantadine and anticholinergics may be useful as treatment of motor symptoms in early and late PD, but since the quality of evidence on efficacy is reduced, they are not first-choice treatments.[3] In addition to motor symptoms, PD is accompanied by a range of different symptoms. Different compounds are used to improve some of these problems.[10][11] Examples are the use of clozapine for psychosis, cholinesterase inhibitors for dementia, modafinil for day somnolence, and atomoxetine for executive dysfunction.[10][11][12]
A preliminary study indicates taking donepezil (Aricept) may help prevent falls in people with Parkinson's. Donepezil boosts the levels of the neurotransmitter acetylcholine, and is currently an approved therapy for the cognitive symptoms of Alzheimer's disease.[13] In the study, participants taking donepezil experienced falls half as often as those taking a placebo, and those who previously fell the most showed the most improvement.[14]
The introduction of clozapine (Clozaril) represents a breakthrough in the treatment of psychotic symptoms of PD. Prior to its introduction, treatment of psychotic symptoms relied on reduction of dopamine therapy or treatment with first generation antipsychotics, all of which worsened motor function. Other atypical antipsychotics useful in treatment include quetiapine (Seroquel), ziprasidone (Geodon), aripiprazole (Abilify), and paliperidone (Invega). Clozapine is believed to have the highest efficacy and lowest risk of extrapyramidal side effect.[12]
Getting medication on time
Parkinson’s patients who do not get the correct medicine at the right time when they are in hospital, (frequently they are in hospital due to unrelated illnesses) sometimes cannot talk or walk. The health of a majority deteriorated due to unsatisfactory medication management when they are in hospital. Parkinson’s UK believes the NHS could save up to £10m a year and improve the care of Parkinson’s patients if mandatory training is introduced for all hospital staff.[15]
Parkinson UK found:
- "Nearly two thirds of people who have Parkinson’s don’t always get their medication on time in hospital."
- "More than three quarters of people with Parkinson’s that we asked reported that their health deteriorated as a result of poor medication management in hospital."
- "Only 21% of respondents told us they got their medication on time without having to remind hospital staff."[16]
Surgery

Treating PD with surgery was once a common practice, but after the discovery of levodopa, surgery was restricted to only a few cases.[17] Studies in the past few decades have led to great improvements in surgical techniques, and surgery is again being used in people with advanced PD for whom drug therapy is no longer sufficient.[17]
Less than 10% of PD sufferers qualify as suitable candidates for a surgical response. The three different mechanisms of surgical response for PD are: ablative surgery, (the irreversible burning or freezing of brain tissue), stimulation surgery or deep brain stimulation (DBS), and transplantation or restorative surgery.[18]
Target areas for DBS or lesions include the thalamus, the globus pallidus (the lesion technique being called pallidotomy), or the subthalamic nucleus.[17]
Neuroablative lesion surgery
Neuroablative lesion surgery locates and destroys, by heat, the parts of the brain associated with producing Parkinsonian neurological symptoms. The procedures generally involve a thalamotomy and/or pallidotomy. A thalamotomy is the destruction of a part of the thalamus, in particular the ventralis intermedius, to suppress tremor in 80-90% of patients. If rigidity and akinesia are apparent, the subthalamis nucleus is then the site of ablation.
A pallidotomy involves the destruction of the globus pallidus, in particular the globus pallidus interna, in patients with Parkinson's who suffer from rigidity and akinesia.
Because it is difficult to accurately measure the amount of tissue to be destroyed, tremors not uncommonly persist through multiple courses of surgery, since tissue is irreversibly damaged and removed and testing smaller areas of tissue is safer to prevent serious complications, such as a stroke or paralysis.. This method has been generally replaced by deep brain surgery.
Deep brain stimulation
Deep brain stimulation (DBS) is presently the most used method of surgical treatment because it does not destroy brain tissue, it is reversible, and it can be tailored to individuals at their particular stage of disease. DBS employs three hardware components: a neurostimulator, also called an implanted pulse generator (IPG), which generates electrical impulses used to modulate neural activity, a lead wire which directs the impulses to a number of metallic electrodes towards the tip of the lead near the stimulation target, and an extension wire that connects the lead to the IPG. The IPG, which is battery-powered and encased in titanium, is traditionally implanted under the collarbone, and is connected by the subcutaneous extension to the lead, which extends from outside the skull under the scalp down into the brain to the target of stimulation. The IPG, or the entire three-component system, are sometimes referred to as a brain pacemaker, due to the precedence and renown of cardiac pacemakers and similarities in the components of both types of systems.
The preoperative targeting of proper implantation sites can be accomplished by the indirect and direct methods. The indirect method uses computer tomography, magnetic resonance imaging, or ventriculography to locate the anterior and posterior commissures and then employs predetermined coordinates and distances from the intercommissural line to define the target area. Subsequent histologically defined atlas maps can also be used to verify the target area. The direct method provides visualization and targeting of deep nuclei by applying stereotactic preoperative MRI, which unlike the indirect method, takes into account the anatomic variation of the nuclei’s size, position, and functional segregation amongst individuals.[19]
Electrophysial functional mapping, a tool used in both methods to verify the target nuclei, has come under scrutiny due to its associated risks of hemorrhages, dysarthria or tetanic contractions. Recently, susceptibility-weighted imaging, a type of MRI, has shown incredible power in its ability to distinguish these deep brain nuclei and is being used in DBS to reduce the overuse of EFM.[20]
DBS is recommended to PD patients without important neuropsychiatric contraindications who suffer motor fluctuations and tremor badly controlled by medication, or to those who are intolerant to medication.[4]
DBS is effective in suppressing symptoms of PD, especially tremor. A recent clinical study led to recommendations on identifying which Parkinson's patients are most likely to benefit from DBS.[4]
Diet
Muscles and nerves that control the digestive process may be affected by PD, so it is common to experience constipation and gastroparesis (food remaining in the stomach for a longer period of time than normal).[21] A balanced diet is recommended to help improve digestion. Diet should include high-fiber foods and plenty of water.[21] Levodopa and proteins use the same transportation system in the intestine and the blood–brain barrier, competing between them for access.[21] When taken together, the consequences of such competition is a reduced effectiveness of the drug.[21] Therefore, when levodopa is introduced, excessive proteins are discouraged, while in advanced stages, additional intake of low-protein products such as bread or pasta is recommended for similar reasons.[21] To minimize interaction with proteins, levodopa is recommended to be taken 30 minutes before meals.[21] At the same time, regimens for PD restrict proteins during breakfast and lunch and are usually taken at dinner.[21] As the disease advances, dysphagia may appear. In such cases, specific measures include the use of thickening agents for liquid intake, special postures when eating, and gastrostomy in the worst cases.[21]
Rehabilitation
Studies of rehabilitation in Parkinson's disease are scarce and are of low quality.[22][23] Partial evidence indicates speech or mobility problems can improve with rehabilitation.[22][23] Regular physical exercise and/or therapy can be beneficial to maintain and improve mobility, flexibility, strength, gait speed, and quality of life.[23] Exercise may also improve constipation. Exercise interventions have been shown to benefit patients with Parkinson’s disease in regards to physical functioning, health-related quality of life, and balance and fall risk. In a review of 14 studies examining the effects of exercise on persons with Parkinson’s disease, no adverse events or side effects occurred following any of the exercise interventions.[24] Five proposed mechanisms by which exercise enhances neuroplasticity are known. Intensive activity maximizes synaptic plasticity; complex activities promote greater structural adaptation; activities that are rewarding increase dopamine levels and therefore promote learning/relearning; dopaminergic neurones are highly responsive to exercise and inactivity (“use it or lose it”); and where exercise is introduced at an early stage of the disease, progression can be slowed.[21][25] One of the most widely practiced treatments for speech disorders associated with Parkinson's disease is the Lee Silverman voice treatment (LSVT), which focuses on increasing vocal loudness and has an intensive approach of one month.[22][26] Speech therapy and specifically LSVT may improve voice and speech function.[22] Occupational therapy (OT) aims to promote health and quality of life by helping people with the disease to participate in as many activities of their daily living as possible.[22] Few studies have been conducted on the effectiveness of OT and their quality is poor, although some indication shows it may improve motor skills and quality of life for the duration of the therapy.[22][27]
For monitoring patients with Parkinson's disease, research teams are examining whether virtual house calls can replace visits to clinical facilities. In a trial of such video visits, patients preferred the remote specialist after 1 year.[28] The home care was considered convenient but requires access to and familiarity with Internet-enabled technologies.
Exercise
Regular physical exercise with or without physiotherapy can be beneficial to maintain and improve mobility, flexibility, strength, gait speed, and quality of life.[23][29] In terms of improving flexibility and range of motion for patients experiencing rigidity, generalized relaxation techniques such as gentle rocking have been found to decrease excessive muscle tension. Other effective techniques to promote relaxation include slow rotational movements of the extremities and trunk, rhythmic initiation, diaphragmatic breathing, and meditation techniques.[30] Common changes in gait associated with the disease such as hypokinesia (slowness of movement), shuffling and decreased arm swing are addressed by a variety of strategies to improve functional mobility and safety. Goals with respect to gait during rehabilitation programs include improving gait speed, base of support, stride length, trunk and arm swing movement. Strategies include utilizing assistive equipment (pole walking and treadmill walking), verbal cueing (manual, visual and auditory), exercises (marching and PNF patterns) and varying environments (surfaces, inputs, open vs. closed).[31]
Strengthening exercises have led to improvements in strength and motor functions in patients with primary muscular weakness and weakness related to inactivity in cases of mild to moderate Parkinson’s disease.[29] Patients perform exercises when at their best, 45 minutes to one hour after medication.[32] An 8-week resistance training study geared towards the lower legs found that patients with Parkinson's Disease gained abdominal strength, and improved in their stride length, walking velocity and postural angles.[33] Also, due to the forward flexed posture and respiratory dysfunctions in advanced Parkinson’s disease, deep diaphragmatic breathing exercises are beneficial for improving chest wall mobility and vital capacity.[34] Exercise may correct constipation.[35]
Exercise training on a vibratory platform, also called whole body vibration (WBV) training, has been recently introduced as a training tool complementing standard physical rehabilitation programs for people with Parkinson’s disease. Compared to no intervention, single sessions of WBV have resulted in improved motor ability, as reflected by Unified Parkinson's Disease Rating Scale (UPDRS) tremor and rigidity scores.[36][37] However, longer-term (3–5 weeks) WBV programs have not led to improved UPDRS motor scores compared to conventional exercises.[38][39] Furthermore, multiple sessions of WBV have failed to enhance mobility measures (i.e., the Timed Up and Go Test and 10-Meter Walking Test) in people with Parkinson’s disease.[38][39] A recent review deemed that the evidence of the effects of WBV training on sensorimotor and functional performance remains inconclusive.[40]
Rhythmic auditory stimulation
Rhythmic auditory stimulation (RAS) is a neurological rehabilitation technique consisting in compensating the loss of motor regulation through an external sensory stimulation, mediated by the sound. This technique relies on the strong interaction between auditory and motor neural system. By synchronizing his footsteps on the emitted sound (that can be "metronome-like" cues or complex music) the patient can improves his gait speed and his stride length.[41]
This rehabilitation technique is usually used by physical and occupational therapist for support rhythmic exercise (nordic walking). Nevertheless, studies show that RAS is also a promising auto-rehabilitation technique for patients, at home.[42]
An electronic device, allegedly based on these statements, was developed and then became available on the market. Albeit there are no medical claims made for this product, its manufacturer hopes to improve mobility problems of people suffering from this disease.[43]
Cuing
Visual, auditory, and somatosensory cuing devices have also been used [44] in conjunction with walking aids to improve gait in individuals with Parkinson’s disease. These cuing strategies have been implemented in an 'app' called Parkinson Home Exercises.[45]
Given the challenge that this clinical population may have with initiating motor movements during gait (e.g., freezing gait) , these devices provide external stimulation to cue for the next step to take place.[46]
Gait training
Gait impairment in people with Parkinson's Disease occurs when they generate an inappropriate stride length.[47]
Task-specific gait training may also lead to long-term gait improvement for patients with Parkinson's disease. Previous research studies have utilized body weight support systems during gait training, where individuals are suspended from an overhead harness with straps around the pelvic girdle as they walk on a treadmill. This form of gait training has been shown to improve long-term walking speed and a shuffling gait following a one-month intervention period.[48]
Studies are also looking at the effect of tai chi on gait performance, and balance in people with Parkinson's Disease.[49][50] The first study concluded that tai chi was ineffective since there was no improvement on gait performance and no improvement on the Part III score of the Unified Parkinson's Disease Rating Scale (UPDRS).[49] The second study found that patients taking tai chi improved on their UPDRS score, Timed Up and Go test, six-minute walk and backwards walking.[50] It did not however, show any improvements on their forward walking or their one leg stance test.[50]
Speech and occupational therapy
One of the most widely practiced treatments for speech disorders associated with Parkinson's disease is the Lee Silverman voice treatment (LSVT).[22][26] Speech therapy and specifically LSVT may improve speech.[22]
A study was conducted to determine if LSVT was beneficial in improving sentence intelligibility of 8 speakers with Parkinson's Disease, according to normal-hearing listeners.[51] The study concluded that after LSVT, there was a significant improvement in the percentage of the words understood by the listeners.[51] Even though the LSVT was not beneficial for 2 of the speakers, the treatment did increase their vocal loudness.[51] Therefore, LSVT has shown that it can improve speech and voice impairments in people with Parkinson's Disease.[51]
People with Parkinson's disease can also develop dysarthria which is characterized by reduced speech intelligibility. Prosodically-based treatments may help.[52]
Occupational therapy aims to promote health and quality of life by helping people with the disease to participate in as much of their daily routine as possible.[22] There is indication that occupational therapy may improve motor skills and quality of life for the duration of the therapy.[22][27]
Music therapy
Studies are considering whether music therapy can have a beneficial effect on people with Parkinson's Disease.[53] A 3-month study investigated whether there was any motor benefit of music therapy and physical therapy on Parkinson's Disease patients, and whether the therapies had any effect on their emotional well being and their quality of life.[53] The music therapy consisted of choral singing, voice exercise and rhythmic and free body movements, whereas the physical therapy consisted of stretching exercises, specific motor tasks and ways to improve balance and gait.[53] The study concluded that music therapy had a beneficial effect on the patient's emotions, it showed an improvement in bradykinesia, and in quality of life.[53] Music therapy however lacked any motor benefit, whereas physical therapy showed that it improved the rigidity of the patients.[53]
Telemedicine
A 2017 one-year randomized controlled trial found that providing remote neurologic care to individuals with Parkinson's Disease in their own homes was feasible and as effective as in-person care. While it can be more difficult for remote caregivers to establish trust while providing remote care, that assessment of video visits in a patient's home found that, after four virtual visits over one year, individuals with Parkinson's Disease preferred their connection with the remote specialist to their local clinician.[54]
Benefits of telemedicine include convenience and cost-effectiveness, as the virtual in-home visits have been found to reduce travel costs and time for patients relative to in-office visits. Some studies have found that the technology supports personalized connections similar to the house calls of the past. Five randomized controlled trials indicated that quality of life was similar or improved for those receiving telemedicine care.[54][55]
Challenges related to telemedicine in treatment of individuals with Parkinson's Disease are related to the technological requirements, as patients and their friends or families must have access to and familiarity with Internet-based technologies.[56] In part because of these technological requirements, studies in the United States have tended to include few participants from ethnic minorities and disproportionately include more highly educated populations. One solution proposed to reduce social and economic barriers to access to remote care is to establish satellite teleneurology clinics in underserved regions.[55][54] Physicians cite barriers with inability to perform a full neurologic exam in addition to technology and reimbursement issues.[57]
New telemedicine technologies being used or evaluated in the context of telemedicine include proprietary wearables, self-sensing and adjusting closed loop systems, robotic technologies, smart devices to detect movements, programs to improve medication adherence, smart home integration, and artificial intelligence or machine learning-based systems.[58]
Palliative care
Palliative care is often required in the final stages of the disease, often when dopaminergic treatments have become ineffective. The aim of palliative care is to achieve the maximum quality of life for the person with the disease and those surrounding him or her. Some central issues of palliative are caring for patients at home while adequate care can be given there, reducing or withdrawing dopaminergic drug intake to reduce drug side effects and complications, preventing pressure ulcers by management of pressure areas of inactive patients, and facilitating the patient's end-of-life decisions for the patient, as well as involved friends and relatives.[59]
Other treatments
Repetitive transcranial magnetic stimulation temporarily improves levodopa-induced dyskinesias.[60] Its full usefulness in PD is an open research field.[61] Different nutrients have been proposed as possible treatments; however, no evidence shows vitamins or food additives improve symptoms.[62] Not enough evidence exists to suggest that acupuncture, and practice of qigong or t'ai chi have any effect on symptoms.[63][64][65] Fava and velvet beans are natural sources of L-DOPA and are taken by many people with PD. While they have shown some effectiveness,[66] their intake is not free of risks. Life-threatening adverse reactions have been described, such as the neuroleptic malignant syndrome.[67][68] Faecal transplants may have a beneficial impact on symptoms.[69]
While not a treatment per se, a wearable device developed by Haiyan Zhang of Microsoft Research Cambridge, can serve to dampen the tremors of a patient's hand and fingers thereby restoring normal functions.[70][71][72] There is also research evaluating the use of telemedicine in movement disorders such as PD.[73] Although remote visits with a specialist can be cost-effective compared to in-person visits, telemedicine requires patients and their caregivers to access to Internet-enabled technologies.[74]
History
The positive albeit modest effects of anticholinergic alkaloids obtained from the plant of the belladona were described during the 19th century by Charcot, Erb, and others. Modern surgery for tremor, consisting of the lesioning of some of the basal ganglia structures was first tried in 1939, and was improved over the following 20 years.[75] Before this date, surgery consisted in lesioning the corticospinal pathway with paralysis instead of tremor as result. Anticholinergics and surgery were the only treaments until the arrival of levodopa, which reduced their use dramatically.[75][76]
Levodopa was first synthesized in 1911 by Casimir Funk, but it received little attention until the mid-20th century.[77] It entered clinical practice in 1967, and the first large study reporting improvements in people with Parkinson's disease resulting from treatment with levodopa was published in 1968. Levodopa brought about a revolution in the management of PD.[77][78] By the late 1980s deep brain stimulation emerged as a possible treatment, and it was approved for clinical use by the FDA in 1997.[79]
Research directions
No new PD treatments are expected in the short term, but several lines of research are active for new treatments.[80] Such research directions include the search of new animal models of the disease, and the potential usefulness of gene therapy, stem cells transplants, and neuroprotective agents.[81]
Animal models
The tragedy of a group of drug addicts in California in the early 1980s who consumed a contaminated and illicitly produced batch of the synthetic opiate MPPP brought to light MPTP as a cause of parkinsonian symptoms.[82] Other predominant toxin-based models employ the insecticide rotenone, the herbicide paraquat, and the fungicide maneb.[83] Models based on toxins are most commonly used in primates. Transgenic rodent models also exist.[84]
Gene therapy
Present treatments of Parkinson's disease provide satisfactory disease control for most early-stage patients.[85] However, present gold-standard treatment of PD using levodopa is associated with motor complications, and does not prevent disease progression.[85] More effective and long-term treatment of PD are urgently needed to control its progression.[85] In vivo gene therapy is a new approach for treatment of PD.[86] The use of somatic-cell gene transfer to alter gene expression in brain neurochemical systems is a novel alternative conventional treatment.[86]
Gene therapy is currently under investigation.[81][87] It involves the use of a noninfectious virus to shuttle a gene into a part of the brain. The gene used leads to the production of an enzyme which helps to manage PD symptoms or protects the brain from further damage.[81]
One of the gene therapy based approach involves gene delivery of neurturin and gilial cell-derived neurotrophic factor (GDNF) to the putamen in patients with advanced Parkinson’s disease.[85] GDNF protects dopamine neurons in vitro and animal models of parkinsonism; neurturin is a structural and functional analogue of GDNF that protected dopamine neuron in animal model of the disease.[85] Despite open-label trials showing benefits of continuous infusion of GDNF, the results were not confirmed in double-blind studies.[85] This may be due to the distribution factor; the trophic factor was not distributed sufficiently throughout the target place.[85]
Another gene therapy of PD involved insertion of the glutamic acid decarboxylase (GAD) into the subthalamic nucleus.[86] GAD enzyme controls GABA productions.[86] In Parkinson’s disease, the activity of both GABA efferents to the subthalamic nucleus and its target within the basal ganglia circuity are affected.[86] This strategy used andeno-associated viral vectoe (AAV2) to deliver GAD to the subthalamic nucleus.[86] The trial was done to compare the effect of bilateral delivery of AAV2-GAD into the subthalamic nucleus with bilateral sham surgery in patients with advanced Parkinson’s disease.[86] The study showed the first success of randomised, double-blind gene therapy trial for a neurodegenerative disease and justified the continued development of AAV2-GAD for treatment of PD.[86]
Neuroprotective treatments
Investigations on neuroprotection are at the forefront of PD research. Currently, no proven neuroprotective agents or treatments are available for PD. While still theoretical, neuroprotective therapy is based on the idea that certain neurons that produce dopamine and are susceptible to premature degeneration and cell death can be protected by the introduction of neuroprotective pharmaceuticals. This protection can occur before any symptoms manifest based on genetic risk, and also during early- or late-stage PD when other treatments have ceased their impact due to the progression of the disease. Accordingly, neuroprotective therapy seeks to delay the introduction of levodopa.
Several molecules have been proposed as potential treatments.[81] However, none of them has been conclusively demonstrated to reduce degeneration.[81] Agents currently under investigation include antiapoptotics (omigapil, CEP-1347), antiglutamatergics, monoamine oxidase inhibitors (selegiline, rasagiline), promitochondrials (coenzyme Q10, creatine), calcium channel blockers (isradipine) and growth factors (GDNF).[81] Preclinical research also targets alpha-synuclein.[80]
Selegiline
Selegiline is in a group of medications called monoamine oxidase type B (MAO-B) inhibitors.[88] Selegiline is used to help control the symptoms of Parkinson's disease in people who are taking levodopa and carbidopa combination (Sinemet). Selegiline may help people with PD by stopping the effects of levodopa/carbidopa from wearing off, and increasing the length of time levodopa/carbidopa continues to control symptoms.
Rasagiline
In response to potentially toxic amphetamine metabolites caused by selegiline, another promising treatment is in MAO B propargyl amine inhibitor rasagiline (N-propargyl-1-R-aminoindan, Azilect((R))). The oral bioavailability of rasagiline is 35%, it reaches T(max) after 0.5–1.0 hours and its half-life is 1.5–3.5 hours. Rasagiline undergoes extensive hepatic metabolism primarily by cytochrome P450 type 1A2 (CYP1A2). Rasagiline is initiated at 1-mg once-daily dose as monotherapy in early PD patients and at 0.5–1.0 mg once-daily as adjunctive to levodopa in advanced PD patients.[89]
Neural transplantation
Since early in the 1980s fetal, porcine, carotid or retinal tissues have been used in cell transplants for PD patients.[81] Although there was initial evidence of mesencephalic dopamine-producing cell transplants being beneficial, the best constructed studies up to date indicate that cell transplants have no effect.[81] An additional significant problem was the excess release of dopamine by the transplanted tissue, leading to dystonias.[90] Stem cell transplants are a main research recent target: they are easy to manipulate and when transplanted into the brains of rodents and monkeys, cells survive and improve behavioral abnormalities of the animals.[81][91] Nevertheless, use of fetal stem cells is controversial.[81] Some have proposed that such controversy may be overcome with the use of induced pluripotent stem cells from adults.[81]
References
- http://www.pdf.org/en/meds_treatments
- http://www.pdf.org/fall08_medications
- The National Collaborating Centre for Chronic Conditions, ed. (2006). "Symptomatic pharmacological therapy in Parkinson's disease". Parkinson's Disease. London: Royal College of Physicians. pp. 59–100. ISBN 978-1-86016-283-1. Guidance was reviewed in 2011 and no changes were made. According to NICE as of July 2014 a revised guidance was under development with anticipated publication in 2017.
- Bronstein JM, Tagliati M, Alterman RL, et al. (October 2010). "Deep Brain Stimulation for Parkinson Disease: An Expert Consensus and Review of Key Issues". Arch Neurol. 68 (2): 165–65. doi:10.1001/archneurol.2010.260. PMC 4523130. PMID 20937936.
- Ceravolo R, Frosini D, Rossi C, Bonuccelli U (December 2009). "Impulse control disorders in Parkinson's disease: definition, epidemiology, risk factors, neurobiology and management". Parkinsonism Relat. Disord. 15 Suppl 4: S111–15. doi:10.1016/S1353-8020(09)70847-8. PMID 20123548.
- Morelli, Micaela; Blandini, Fabio; Simola, Nicola; Hauser, Robert A. (2012). "A2AReceptor Antagonism and Dyskinesia in Parkinson's Disease". Parkinson's Disease. 2012: 489853. doi:10.1155/2012/489853. ISSN 2090-8083. PMC 3382949. PMID 22754707.
- Armentero, Marie Therese; Pinna, Annalisa; Ferré, Sergi; Lanciego, José Luis; Müller, Christa E.; Franco, Rafael (December 2011). "Past, present and future of A2A adenosine receptor antagonists in the therapy of Parkinson's disease". Pharmacology & Therapeutics. 132 (3): 280–299. doi:10.1016/j.pharmthera.2011.07.004. ISSN 0163-7258. PMC 3205226. PMID 21810444.
- Goldenberg MM (October 2008). "Medical management of Parkinson's disease". P & T. 33 (10): 590–606. PMC 2730785. PMID 19750042.
- Samii A, Nutt JG, Ransom BR (May 2004). "Parkinson's disease". Lancet. 363 (9423): 1783–93. doi:10.1016/S0140-6736(04)16305-8. PMID 15172778.
- Warner, Carly B.; Ottman, Andreina A.; Brown, Jamie N. (December 2018). "The Role of Atomoxetine for Parkinson Disease-Related Executive Dysfunction: A Systematic Review". Journal of Clinical Psychopharmacology. 38 (6): 627–631. doi:10.1097/JCP.0000000000000963. ISSN 1533-712X. PMID 30346335.
- The National Collaborating Centre for Chronic Conditions, ed. (2006). "Non-motor features of Parkinson's disease". Parkinson's Disease. London: Royal College of Physicians. pp. 113–33. ISBN 978-1-86016-283-1.
- Hasnain M, Vieweg WV, Baron MS, Beatty-Brooks M, Fernandez A, Pandurangi AK (July 2009). "Pharmacological management of psychosis in elderly patients with parkinsonism". Am. J. Med. 122 (7): 614–22. doi:10.1016/j.amjmed.2009.01.025. PMID 19559160.
- Donepezil (Aricept) Reduces Falls in People with Parkinson’s. Parkinson's Disease Foundation Science News. 11 November 2010.
- Chung, KA.; Lobb, B. M.; Nutt, J. G.; Horak, F. B. (October 2010). "Effects of a central cholinesterase inhibitor on reducing falls in Parkinson disease". Neurology. 75 (10): 1263–69. doi:10.1212/WNL.0b013e3181f6128c. PMC 3013493. PMID 20810998.
- Boris Johnson's mother exits Parkinson's campaign after No 10 intervention The Guardian
- Get It On Time
- The National Collaborating Centre for Chronic Conditions, ed. (2006). "Surgery for Parkinson's disease". Parkinson's Disease. London: Royal College of Physicians. pp. 101–11. ISBN 978-1-86016-283-1.
- Parkinson's disease surgery neurology Channel. Retrieved on 2010-02-02
- Nolte, 2012
- Abosch, 2010
- Barichella M, Cereda E, Pezzoli G (October 2009). "Major nutritional issues in the management of Parkinson's disease". Mov. Disord. 24 (13): 1881–92. doi:10.1002/mds.22705. hdl:2434/67795. PMID 19691125.
- The National Collaborating Centre for Chronic Conditions, ed. (2006). "Other key interventions". Parkinson's Disease. London: Royal College of Physicians. pp. 135–46. ISBN 978-1-86016-283-1.
- Goodwin VA, Richards SH, Taylor RS, Taylor AH, Campbell JL (April 2008). "The effectiveness of exercise interventions for people with Parkinson's disease: a systematic review and meta-analysis". Mov. Disord. 23 (5): 631–40. doi:10.1002/mds.21922. PMID 18181210.
- Goodwin V. A., Richards S. H., Taylor R. S., Taylor A. H., Campbell J. L. (2008). "The effectiveness of exercise interventions for people with Parkinson's disease: a systematic review and meta-analysis". Movement Disorders. 23 (5): 631–40. doi:10.1002/mds.21922. PMID 18181210.CS1 maint: multiple names: authors list (link)
- Fox CM, Ramig LO, Ciucci MR, Sapir S, McFarland DH, Farley BG (2006). "The science and practice of LSVT/LOUD: neural plasticityprincipled approach to treating individuals with Parkinson's disease and other neurological disorders". Semin Speech Lang. 27 (4): 283–299. doi:10.1055/s-2006-955118. PMID 17117354.
- Fox CM, Ramig LO, Ciucci MR, Sapir S, McFarland DH, Farley BG (November 2006). "The science and practice of LSVT/LOUD: neural plasticity-principled approach to treating individuals with Parkinson disease and other neurological disorders". Seminars in Speech and Language. 27 (4): 283–99. doi:10.1055/s-2006-955118. PMID 17117354.
- Dixon L, Duncan D, Johnson P, et al. (2007). Deane K (ed.). "Occupational therapy for patients with Parkinson's disease". Cochrane Database Syst Rev (3): CD002813. doi:10.1002/14651858.CD002813.pub2. PMID 17636709.
- Dorsey, E. Ray; Glidden, Alistair M.; Holloway, Melissa R.; Birbeck, Gretchen L.; Schwamm, Lee H. (May 2018). "Teleneurology and mobile technologies: the future of neurological care". Nature Reviews Neurology. 14 (5): 285–297. doi:10.1038/nrneurol.2018.31. ISSN 1759-4758. PMID 29623949.
- Roeder, Luisa; Costello, Joseph T.; Smith, Simon S.; Stewart, Ian B.; Kerr, Graham K. (2015-07-06). "Effects of Resistance Training on Measures of Muscular Strength in People with Parkinson's Disease: A Systematic Review and Meta-Analysis". PLoS ONE. 10 (7): e0132135. doi:10.1371/journal.pone.0132135. PMC 4492705. PMID 26146840.
- O'Sullivan & Schmitz 2007, pp. 873, 876
- O'Sullivan & Schmitz 2007, p. 879
- O'Sullivan & Schmitz 2007, p. 877
- Scandalis TA, Bosak A, Berliner JC, Helman LL, Wells MR (2001). "Resistance Training and Gait Function in Patients with Parkinson's Disease". Am J Phys Med Rehabil. 80 (1): 38–43. doi:10.1097/00002060-200101000-00011. PMID 11138953.
- O'Sullivan & Schmitz 2007, p. 880
- Barichella, M; Cereda, E; Pezzoli, G (Oct 15, 2009). "Major nutritional issues in the management of Parkinson's disease". Movement Disorders. 24 (13): 1881–92. doi:10.1002/mds.22705. hdl:2434/67795. PMID 19691125.
- Haas CT, Turbanski S, Kessler K, Schmidtbleicher D (2006). "The effects of random whole-body-vibration on motor symptoms in Parkinson's disease". NeuroRehabilitation. 21 (1): 29–36. PMID 16720935.
- King LK, Almeida QJ, Ahonen H (2009). "Short-term effects of vibration therapy on motor impairments in Parkinson's disease". NeuroRehabilitation. 25 (4): 297–306. doi:10.3233/NRE-2009-0528. PMID 20037223.
- Arias P, Chouza M, Vivas J, Cudeiro J (2009). "Effect of whole body vibration in Parkinson's disease: a controlled study". Movement Disorders. 24 (6): 891–898. doi:10.1002/mds.22468. hdl:2183/14508. PMID 19199362.
- Ebersbach G, Edler D, Kaufhold O, Wissel J (2008). "Whole body vibration versus conventional physiotherapy to improve balance and gait in Parkinson's disease". Archives of Physical Medicine and Rehabilitation. 89 (3): 399–403. doi:10.1016/j.apmr.2007.09.031. PMID 18295614.
- Sitjà Rabert M, Rigau Comas D, Fort Vanmeerhaeghe A, Santoyo Medina C, Roqué I, Figuls M, Romero-Rodríguez D, Bonfill Cosp X (2012). "Whole-body vibration training for patients with neurodegenerative disease". Cochrane Database of Systematic Reviews. 15 (2): CD009097. doi:10.1002/14651858.cd009097.pub2. PMID 22336858.
- Spaulding, Sandi J., Brittany Barber, Morgan Colby, Bronwyn Cormack, Tanya Mick, et Mary E. Jenkins (2013). "Cueing and Gait Improvement among People with Parkinson's Disease: A Meta-Analysis". Archives of Physical Medicine and Rehabilitation. 94 (3): 562–70. doi:10.1016/j.apmr.2012.10.026. PMID 23127307.CS1 maint: multiple names: authors list (link)
- Bryant, M. S., D. H. Rintala, E. C. Lai, et E. J. Protas (2009). "An Evaluation of Self-Administration of Auditory Cueing to Improve Gait in People with Parkinson's Disease". Clinical Rehabilitation. 23 (5): 1078–85. doi:10.1080/17483100903038576. PMC 2877128. PMID 19565381.CS1 maint: multiple names: authors list (link)
- Jane, Hanks (4 Apr 2017). "Potential good news for Parkinson's sufferers". The Connexion. Retrieved 2018-06-09.
- van Wegen et al 2006; Nieuwboer et al. 2007
- "Parkinson Home Exercises App". Efox.nl. European Foundation for Health and Exercise. Retrieved 4 December 2015.
- Pongmala, C., Suputtitada, A. & Sriyuthsak, M. (2010). The study of cuing devices by using visual, auditory and somatosensory stimuli for improving gait in Parkinson’s patients. International Conference on Bioinformatics and Biomedical Technology
- Morris ME, Iansek R, Matyas TA, Summers JJ (1996). "Stride length regulation in Parkinson's disease.Normalization strategies and underlying mechanisms". Brain. 119 (2): 551–68. doi:10.1093/brain/119.2.551. PMID 8800948.
- Miyai I.; Fujimoto Y.; Yamamoto H.; et al. (2002). "Long-term effect of body weight-supported treadmill training in Parkinson's disease: a randomized controlled trial". Arch Phys Med Rehabil. 83 (10): 1370–73. doi:10.1053/apmr.2002.34603. PMID 12370870.
- Amano S, Nocera JR, Vallabhajosula S, Juncos JL, Gregor RJ, Waddell DE, Wolf SL, Hass CJ (2013). "The effect of Tai Chi exercise on gait initiation and gait performance in persons with Parkinson's Disease". Parkinsonism Relat Disord. 19 (11): 955–60. doi:10.1016/j.parkreldis.2013.06.007. PMC 3825828. PMID 23835431.
- Hackney ME, Earhart GM (2008). "Tai Chi improves balance and mobility in people with Parkinson disease". Gait & Posture. 28 (3): 456–60. doi:10.1016/j.gaitpost.2008.02.005. PMC 2552999. PMID 18378456.
- Cannito MP, Suiter DM, Beverly D, Chorna L, Wolf T, Pfeiffer RM (2012). "Sentence Intelligibility Before and After Voice Treatment in Speakers With Idiopathic Parkinson's Disease". Journal of Voice. 26 (2): 214–19. doi:10.1016/j.jvoice.2011.08.014. PMID 22209057.
- Tjaden, K (2008). "Speech and swallowing in parkinson's disease". Top Geriatric Rehabilitation. 28 (2): 115–26. doi:10.1097/01.TGR.0000318899.87690.44. PMC 2784698. PMID 19946386.
- Pacchetti C, Mancini F, Aglieri R, Fundaro C, Martignoni E, Nappi G (2000). "Active Music Therapy in Parkinson's Disease: An Integrative Method for Motor and Emotional Rehabilitation". Psychosomatic Medicine. 62 (2): 386–93. CiteSeerX 10.1.1.555.3509. doi:10.1097/00006842-200005000-00012. PMID 10845352.
- Beck, Christopher A.; Beran, Denise B.; Biglan, Kevin M.; Boyd, Cynthia M.; Dorsey, E. Ray; Schmidt, Peter N.; Simone, Richard; Willis, Allison W.; Galifianakis, Nicholas B. (2017-09-12). "National randomized controlled trial of virtual house calls for Parkinson disease". Neurology. 89 (11): 1152–1161. doi:10.1212/WNL.0000000000004357. ISSN 0028-3878. PMC 5595275. PMID 28814455.
- Dorsey, E. Ray; Achey, Meredith A.; Beck, Christopher A.; Beran, Denise B.; Biglan, Kevin M.; Boyd, Cynthia M.; Schmidt, Peter N.; Simone, Richard; Willis, Allison W. (July 2016). "National Randomized Controlled Trial of Virtual House Calls for People with Parkinson's Disease: Interest and Barriers". Telemedicine and E-Health. 22 (7): 590–598. doi:10.1089/tmj.2015.0191. ISSN 1530-5627. PMC 4939367. PMID 26886406.
- Beck, Christopher A.; Beran, Denise B.; Biglan, Kevin M.; Boyd, Cynthia M.; Dorsey, E. Ray; Schmidt, Peter N.; Simone, Richard; Willis, Allison W.; Galifianakis, Nicholas B. (2017-09-12). "National randomized controlled trial of virtual house calls for Parkinson disease". Neurology. 89 (11): 1152–1161. doi:10.1212/WNL.0000000000004357. ISSN 1526-632X. PMC 5595275. PMID 28814455.
- Mammen, Jennifer R.; Elson, Molly J.; Java, James J.; Beck, Christopher A.; Beran, Denise B.; Biglan, Kevin M.; Boyd, Cynthia M.; Schmidt, Peter N.; Simone, Richard (April 2018). "Patient and Physician Perceptions of Virtual Visits for Parkinson's Disease: A Qualitative Study". Telemedicine and E-Health. 24 (4): 255–267. doi:10.1089/tmj.2017.0119. ISSN 1530-5627. PMID 28787250.
- Dorsey, E. Ray; Vlaanderen, Floris P.; Engelen, Lucien JLPG; Kieburtz, Karl; Zhu, William; Biglan, Kevin M.; Faber, Marjan J.; Bloem, Bastiaan R. (September 2016). "Moving Parkinson care to the home: Moving Parkinson Care To The Home". Movement Disorders. 31 (9): 1258–1262. doi:10.1002/mds.26744. PMC 5014631. PMID 27501323.
- The National Collaborating Centre for Chronic Conditions, ed. (2006). "Palliative care in Parkinson's disease". Parkinson's Disease. London: Royal College of Physicians. pp. 147–51. ISBN 978-1-86016-283-1.
- Koch G (2010). "rTMS effects on levodopa induced dyskinesias in Parkinson's disease patients: searching for effective cortical targets". Restor. Neurol. Neurosci. 28 (4): 561–68. doi:10.3233/RNN-2010-0556. PMID 20714078.
- Platz T, Rothwell JC (2010). "Brain stimulation and brain repair – rTMS: from animal experiment to clinical trials – what do we know?". Restor. Neurol. Neurosci. 28 (4): 387–98. doi:10.3233/RNN-2010-0570. PMID 20714064.
- Suchowersky O, Gronseth G, Perlmutter J, Reich S, Zesiewicz T, Weiner WJ (April 2006). "Practice Parameter: neuroprotective strategies and alternative therapies for Parkinson disease (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology". Neurology. 66 (7): 976–82. doi:10.1212/01.wnl.0000206363.57955.1b. PMID 16606908.
- Lee MS, Lam P, Ernst E (December 2008). "Effectiveness of tai chi for Parkinson's disease: a critical review". Parkinsonism Relat. Disord. 14 (8): 589–94. doi:10.1016/j.parkreldis.2008.02.003. PMID 18374620.
- Lee MS, Ernst E (January 2009). "Qigong for movement disorders: A systematic review". Mov. Disord. 24 (2): 301–03. doi:10.1002/mds.22275. PMID 18973253.
- Lee MS, Shin BC, Kong JC, Ernst E (August 2008). "Effectiveness of acupuncture for Parkinson's disease: a systematic review". Mov. Disord. 23 (11): 1505–15. doi:10.1002/mds.21993. PMID 18618661.
- Katzenschlager R, Evans A, Manson A, et al. (2004). "Mucuna pruriens in Parkinson's disease: a double blind clinical and pharmacological study". J. Neurol. Neurosurg. Psychiatry. 75 (12): 1672–77. doi:10.1136/jnnp.2003.028761. PMC 1738871. PMID 15548480.
- Ladha SS, Walker R, Shill HA (May 2005). "Case of neuroleptic malignant-like syndrome precipitated by abrupt fava bean discontinuance". Mov. Disord. 20 (5): 630–31. doi:10.1002/mds.20380. PMID 15719433.
- Raguthu L, Varanese S, Flancbaum L, Tayler E, Di Rocco A (October 2009). "Fava beans and Parkinson's disease: useful 'natural supplement' or useless risk?". Eur. J. Neurol. 16 (10): e171. doi:10.1111/j.1468-1331.2009.02766.x. PMID 19678834.
- "Faecal transplant eases symptoms of Parkinson's".
- Jones, Brad (December 8, 2016). "Wearable Device Helps Steady Hand of Designer Who Has Parkinson's Disease". digitaltrends.com.
- Thomas, Josh (December 9, 2016). "Cambridge inventor helps Parkinson's disease suffer to write again". cambridge-news.co.uk. Cambridgeshire, England: Cambridge News. Retrieved 15 December 2016.
- Mann, Tanveer (8 December 2016). "Woman with Parkinson's can write again using incredible invention". metro.co.uk. Retrieved 15 December 2016.
- Ben-Pazi, H.; Browne, P.; Chan, P.; Cubo, E.; Guttman, M.; Hassan, A.; Hatcher-Martin, J.; Mari, Z.; Moukheiber, E. (2018-04-13). "The Promise of Telemedicine for Movement Disorders: an Interdisciplinary Approach". Current Neurology and Neuroscience Reports. 18 (5): 26. doi:10.1007/s11910-018-0834-6. ISSN 1534-6293. PMID 29654523.
- Dorsey, E. Ray; Glidden, Alistair M.; Holloway, Melissa R.; Birbeck, Gretchen L.; Schwamm, Lee H. (May 2018). "Teleneurology and mobile technologies: the future of neurological care". Nature Reviews. Neurology. 14 (5): 285–297. doi:10.1038/nrneurol.2018.31. ISSN 1759-4766. PMID 29623949.
- Lanska DJ (2010). Chapter 33: the history of movement disorders. Handb Clin Neurol. Handbook of Clinical Neurology. 95. pp. 501–46. doi:10.1016/S0072-9752(08)02133-7. ISBN 9780444520098. PMID 19892136.
- Guridi J, Lozano AM (November 1997). "A brief history of pallidotomy". Neurosurgery. 41 (5): 1169–80, discussion 1180–83. doi:10.1097/00006123-199711000-00029. PMID 9361073.
- Fahn S (2008). "The history of dopamine and levodopa in the treatment of Parkinson's disease". Mov. Disord. 23 Suppl 3: S497–508. doi:10.1002/mds.22028. PMID 18781671.
- Hornykiewicz O (2002). "L-DOPA: from a biologically inactive amino acid to a successful therapeutic agent". Amino Acids. 23 (1–3): 65–70. doi:10.1007/s00726-001-0111-9. PMID 12373520.
- Coffey RJ (March 2009). "Deep brain stimulation devices: a brief technical history and review". Artif Organs. 33 (3): 208–20. doi:10.1111/j.1525-1594.2008.00620.x. PMID 18684199.
- Dimond PF (2010-08-16), "No New Parkinson Disease Drug Expected Anytime Soon", GEN news highlights, GEN-Genetic Engineering & Biotechnology News, retrieved 2010-10-25
- Obeso JA, Rodriguez-Oroz MC, Goetz CG, et al. (May 2010). "Missing pieces in the Parkinson's disease puzzle". Nat Med. 16 (6): 653–61. doi:10.1038/nm.2165. PMID 20495568.
- Langston JW, Ballard P, Tetrud JW, Irwin I (February 1983). "Chronic Parkinsonism in humans due to a product of meperidine-analog synthesis". Science. 219 (4587): 979–80. doi:10.1126/science.6823561. PMID 6823561.
- Cicchetti F, Drouin-Ouellet J, Gross RE (September 2009). "Environmental toxins and Parkinson's disease: what have we learned from pesticide-induced animal models?". Trends Pharmacol. Sci. 30 (9): 475–83. doi:10.1016/j.tips.2009.06.005. PMID 19729209.
- Harvey BK, Wang Y, Hoffer BJ (2008). Transgenic rodent models of Parkinson's disease. Acta Neurochir. Suppl. Acta Neurochirurgica Supplementum. 101. pp. 89–92. doi:10.1007/978-3-211-78205-7_15. ISBN 978-3-211-78204-0. PMC 2613245. PMID 18642640.
- Marks WJ, Bartus RT, Siffert J, Davis CS, Lozano A, Boulis N, Vitek J, Stacy M, Turner D, Verhagen L, Bakay R, Watts R, Guthrie B, Jankovic J, Simpson R, Tagliati M, Alterman R, Stern M, Baltuch G, Starr PA, Larson PS, Ostrem JL, Nutt J, Kieburtz K, Kordower JH, Olanow CW (Dec 2010). "Gene delivery of AAV2-neurturin for Parkinson's disease: a double-blind, randomised, controlled trial". Lancet Neurology. 9 (12): 1164–72. doi:10.1016/S1474-4422(10)70254-4. PMID 20970382. CN-00772567.
- LeWitt PA, Rezai AR, Leehey MA, Ojemann SG, Flaherty AW, Eskandar EN, Kostyk SK, Thomas K, Sarkar A, Siddiqui MS, Tatter SB, Schwalb JM, Poston KL, Henderson JM, Kurlan RM, Richard IH, Van Meter L, Sapan CV, During MJ, Kaplitt MG, Feigin A (Apr 2011). "AAV2-GAD gene therapy for advanced Parkinson's disease: a double-blind, sham-surgery controlled, randomised trial". Lancet Neurology. 10 (4): 309–19. doi:10.1016/S1474-4422(11)70039-4. PMID 21419704. CN-00786419.
- Feng, LR, Maguire-Zeiss KA (2010). "Gene Therapy in Parkinson's Disease: Rationale and Current Status". CNS Drugs. 24 (3): 177–92. doi:10.2165/11533740-000000000-00000. PMC 2886503. PMID 20155994.CS1 maint: multiple names: authors list (link)
- Selegiline Information MedLine Plus. Retrieved on 2010-02-02
- Treat Parkinson Disease Effectively Archived 2010-02-08 at the Wayback Machine Retrieved on 2010-02-02
- Redmond DE (October 2002). "Cellular replacement therapy for Parkinson's disease – where we are today?". The Neuroscientist. 8 (5): 457–88. doi:10.1177/107385802237703. PMID 12374430.
- "Stem Cell Research Aims to Tackle Parkinson's Disease". Retrieved 2010-04-16.
External links
- Parkinson's Medication Chart at the Parkinson's Disease Foundation
- PDtrials
- Find What Treatments Are Possible