Anosmia
Anosmia, also known as smell blindness, is the loss of the ability to detect one or more smells.[1][2] Anosmia may be temporary or permanent. It differs from hyposmia which is a decreased sensitivity to some or all smells.[2]
| Anosmia | |
|---|---|
| Other names | Loss of smell, smell blindness,[1] odor blindness |
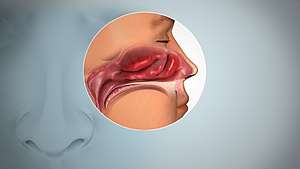 | |
| Inflamed nasal mucosa causing anosmia | |
| Pronunciation |
|
| Specialty | Otorhinolaryngology |
| Types | Partial, total[2] |
Anosmia is due to a number of factors, including an inflammation of the nasal mucosa, blockage of nasal passages or a destruction of one temporal lobe. Inflammation is due to chronic mucosa changes in the paranasal sinus lining and the middle and superior turbinates.
When anosmia is caused by inflammatory changes in the nasal passageways, it is treated simply by reducing inflammation.[3] It can be caused by chronic meningitis and neurosyphilis that would increase intracranial pressure over a long period of time,[4] and in some cases by ciliopathy[5] including ciliopathy due to primary ciliary dyskinesia (Kartagener syndrome, Afzelius' syndrome or Siewert's syndrome).[6]
The term is from the New Latin anosmia, based on Ancient Greek ἀν- (an-) + ὀσμή (osmḗ, "smell". A related term, hyposmia, refers to a decreased ability to smell, while hyperosmia refers to an increased ability to smell. Some people may be anosmic for one particular odor. This is known as "specific anosmia". The absence of the sense of smell from birth is called congenital anosmia.
Signs and symptoms
Anosmia can have a number of harmful effects. People with sudden onset anosmia may find food less appetizing, though congenital anosmics rarely complain about this, and none report a loss in weight. Loss of smell can also be dangerous because it hinders the detection of gas leaks, fire, and spoiled food. The common view of anosmia as trivial can make it more difficult for a patient to receive the same types of medical aid as someone who has lost other senses, such as hearing or sight.
Many experience one sided loss of smell, often as a result of minor head trauma. This type of anosmia is normally only detected if both of the nostrils are tested separately. Using this method of testing each nostril separately will often show a reduced or even completely absent sense of smell in either one nostril or both, something which is often not revealed if both nostrils are simultaneously tested.[7]
Losing an established and sentimental smell memory (e.g. the smell of grass, of the grandparents' attic, of a particular book, of loved ones, or of oneself) has been known to cause feelings of depression.[8]
Loss of olfaction may lead to the loss of libido, though this usually does not apply to congenital anosmics.[8]
Often people who have congenital anosmia report that they pretended to be able to smell as children because they thought that smelling was something that older/mature people could do, or did not understand the concept of smelling but did not want to appear different from others. When children get older, they often realize and report to their parents that they do not actually possess a sense of smell, often to the surprise of their parents.
A study done on patients suffering from anosmia found that when testing both nostrils, there was no anosmia revealed; however, when testing each nostril individually, tests showed that the sense of smell was usually affected in only one of the nostrils as opposed to both. This demonstrated that unilateral anosmia is not uncommon in anosmia patients.[7]
Causes
A temporary loss of smell can be caused by a blocked nose or infection. In contrast, a permanent loss of smell may be caused by death of olfactory receptor neurons in the nose or by brain injury in which there is damage to the olfactory nerve or damage to brain areas that process smell (see olfactory system). The lack of the sense of smell at birth, usually due to genetic factors, is referred to as congenital anosmia. Family members of the patient suffering from congenital anosmia are often found with similar histories; this suggests that the anosmia may follow an autosomal dominant pattern.[9] Anosmia may very occasionally be an early sign of a degenerative brain disease such as Parkinson's disease and Alzheimer's disease.
Another specific cause of permanent loss could be from damage to olfactory receptor neurons because of use of certain types of nasal spray; i.e., those that cause vasoconstriction of the nasal microcirculation. To avoid such damage and the subsequent risk of loss of smell, vasoconstricting nasal sprays should be used only when absolutely necessary and then for only a short amount of time. Non-vasoconstricting sprays, such as those used to treat allergy-related congestion, are safe to use for prescribed periods of time.[10] Anosmia can also be caused by nasal polyps. These polyps are found in people with allergies, histories of sinusitis & family history. Individuals with cystic fibrosis often develop nasal polyps.
Amiodarone is a drug used in the treatment of arrhythmias of the heart. A clinical study demonstrated that the use of this drug induced anosmia in some patients. Although rare, there was a case in which a 66-year-old male was treated with Amiodarone for ventricular tachycardia. After the use of the drug he began experiencing olfactory disturbance, however after decreasing the dosage of Amiodarone, the severity of the anosmia decreased accordingly hence correlating the use of Amiodarone to the development of anosmia.[11]
List of causes
- Upper respiratory tract infection (e.g., sinusitis or the common cold)[12]
- Nasal polyps[13]
- Idiopathic hypogonadotropic hypogonadism
- Hypothyroidism
- Head trauma, damage to the ethmoid bone[14]
- Dementia with Lewy bodies
- Tumors of the frontal lobe
- Antibiotics
- Fibromyalgia
- Multiple sclerosis
- Hypoglycaemia
- Diabetes
- Asthma or Allergy
- Hayfever
- Chronic obstructive pulmonary disease (COPD)
- Long term alcoholism
- Cushing's syndrome
- Exposure to a chemical that burns the inside of the nose
- Stroke
- Epilepsy
- Radiation therapy to the head and neck
- Liver or kidney disease
- Parkinson's disease[15]
- Alzheimer's disease[16]
- Toxins (especially acrylates, methacrylates[17] and cadmium[18][19])
- Old age[20]
- Kallmann syndrome
- Primary ciliary dyskinesia
- Post-perfusion syndrome
- Laryngectomy with permanent tracheostomy
- Esthesioneuroblastoma is an exceedingly rare cancerous tumor that originates in or near the olfactory nerve. Symptoms are anosmia (loss of sense of smell) often accompanied by chronic sinusitis.[21]
- Intranasal drug use
- Samter's triad also known as AERD (aspirin exacerbated respiratory disease)
- Foster Kennedy syndrome
- Cadmium poisoning
- Smoking
- Neurotropic virus[22]
- Schizophrenia[23]
- Pernicious anemia
- Zinc deficiency
- Bell's Palsy or nerve paralysis and damage
- Idiopathic intracranial hypertension
- Suprasellar meningioma
- Refsum's disease
- Adrenergic agonists or withdrawal from alpha blockers (vasoconstriction)
- Sarcoidosis[24]
- Zinc-based intranasal cold products, including remedies labelled as "homeopathic"[25]
- Chronic atrophic rhinitis
- Paget's disease of bone[26]
- Cerebral aneurysm[27]
- Granulomatosis with polyangiitis
- Primary amoebic meningoencephalitis
- Myasthenia gravis[28]
- Idiopathic anosmia (cause cannot be determined)[29]
- Snakebite[30]
Diagnosis
Anosmia can be diagnosed by doctors by using acetylcysteine tests. Doctors will begin with a detailed elicitation of history. Then the doctor will ask for any related injuries in relation to anosmia which could include upper respiratory infections or head injury. Psychophysical Assessment of order and taste identification can be used to identify anosmia. A nervous system examination is performed to see if the cranial nerves are damaged.[31] The diagnosis as well as the degree of impairment can now be tested much more efficiently and effectively than ever before thanks to "smell testing kits" that have been made available as well as screening tests which use materials that most clinics would readily have.[32] Occasionally, after accidents, there is a change in a patient's sense of smell. Particular smells that were present before are no longer present. On occasion, after head traumas, there are patients who have unilateral anosmia. The sense of smell should be tested individually in each nostril.[7]
Many cases of congenital anosmia remain unreported and undiagnosed. Since the disorder is present from birth the individual may have little or no understanding of the sense of smell, hence is unaware of the deficit.[33] It may also lead to reduction of appetite.[34]
Treatment
Though anosmia caused by brain damage cannot be treated, anosmia caused by inflammatory changes in the mucosa may be treated with glucocorticoids. Reduction of inflammation through the use of oral glucocorticoids such as prednisone, followed by long term topical glucocorticoid nasal spray, would easily and safely treat the anosmia. A prednisone regimen is adjusted based on the degree of the thickness of mucosa, the discharge of oedema and the presence or absence of nasal polyps.[3] However, the treatment is not permanent and may have to be repeated after a short while.[3] Together with medication, pressure of the upper area of the nose must be mitigated through aeration and drainage.[35]
Anosmia caused by a nasal polyp may be treated by steroidal treatment or removal of the polyp.[36]
Although very early in development, gene therapy has restored a sense of smell in mice with congenital anosmia when caused by ciliopathy. In this case a genetic condition had affected cilia in their bodies which normally enabled them to detect air-borne chemicals, and an adenovirus was used to implant a working version of the IFT88 gene into defective cells in the nose, which restored the cilia and allowed a sense of smell.[37][38]
See also
- Phantosmia
- Hyperosmia
- Hyposmia
- Parosmia
- Anosmia Awareness Day
- Zicam, a medicine that caused some users to permanently lose their sense of smell
References
- Coon, Dennis; Mitterer, John (2006). Introduction to Psychology: Gateways to Mind and Behavior. Cengage Learning. p. 174. ISBN 9780495091554.
- Jones, Nicholas (2010). Practical Rhinology. CRC Press. p. 25. ISBN 9781444108613.
- Knight, Allan (1988). "Anosmia". The Lancet. 332 (8609): 512. doi:10.1016/S0140-6736(88)90160-2. PMID 2900434.
- "Anosmia". The Lancet. 241 (6228): 55. 1943. doi:10.1016/S0140-6736(00)89085-6.
- Impact of Defective Cilia
- Ul Hassan A, Hassan G, Khan SH, Rasool Z, Abida A (January 2009). "Ciliopathy with special emphasis on kartageners syndrome". International Journal of Health Sciences. 3 (1): 65–9. PMC 3068795. PMID 21475513.
- Harvey, Peter (February 2006). "Anosmia". Practical Neurology. 6 (1): 65.
- Heald, Claire (December 27, 2006). "Sense and scent ability". BBC News. Retrieved April 25, 2010.
- Waguespack, R. W. (1992). "Congenital Anosmia". Archives of Otolaryngology–Head & Neck Surgery. 118 (1): 10. doi:10.1001/archotol.1992.01880010012002.
- Preventing Anosmia from Intranasal Zinc Administration
- Maruyama T, Yasuda S, Odashiro K, Kaji Y, Harada M (November 2007). "Anosmia induced by amiodarone". The American Journal of Medicine. 120 (11): e9. doi:10.1016/j.amjmed.2006.08.029. PMID 17976411.
- Doty RL, Mishra A (March 2001). "Olfaction and its alteration by nasal obstruction, rhinitis, and rhinosinusitis". The Laryngoscope. 111 (3): 409–23. doi:10.1097/00005537-200103000-00008. PMID 11224769.
- Ta NH (2019). "Will we ever cure nasal polyps?". Annals of the Royal College of Surgeons of England. 101 (1): 35–39. doi:10.1308/rcsann.2018.0149. PMC 6303820. PMID 30286644.
- Doty RL, Yousem DM, Pham LT, Kreshak AA, Geckle R, Lee WW (September 1997). "Olfactory dysfunction in patients with head trauma". Archives of Neurology. 54 (9): 1131–40. doi:10.1001/archneur.1997.00550210061014. PMID 9311357.
- Doty RL, Deems DA, Stellar S (August 1988). "Olfactory dysfunction in parkinsonism: a general deficit unrelated to neurologic signs, disease stage, or disease duration". Neurology. 38 (8): 1237–44. doi:10.1212/WNL.38.8.1237. PMID 3399075.
- Murphy, Claire (1999). "Loss of Olfactory Function in Dementing Disease". Physiology & Behavior. 66 (2): 177–82. doi:10.1016/S0031-9384(98)00262-5. PMID 10336141.
- Schwartz BS, Doty RL, Monroe C, Frye R, Barker S (May 1989). "Olfactory function in chemical workers exposed to acrylate and methacrylate vapors". American Journal of Public Health. 79 (5): 613–8. doi:10.2105/AJPH.79.5.613. PMC 1349504. PMID 2784947.
- Rose CS, Heywood PG, Costanzo RM (June 1992). "Olfactory impairment after chronic occupational cadmium exposure". Journal of Occupational Medicine. 34 (6): 600–5. PMID 1619490.
- Rydzewski B, Sułkowski W, Miarzyńska M (1998). "Olfactory disorders induced by cadmium exposure: a clinical study". International Journal of Occupational Medicine and Environmental Health. 11 (3): 235–45. PMID 9844306.
- Doty RL, Shaman P, Applebaum SL, Giberson R, Siksorski L, Rosenberg L (December 1984). "Smell identification ability: changes with age". Science. 226 (4681): 1441–3. Bibcode:1984Sci...226.1441D. doi:10.1126/science.6505700. PMID 6505700.
- Somenek, Michael (October 30, 2009). Harris, Jules E (ed.). "Esthesioneuroblastoma". eMedicine.
- Seo BS, Lee HJ, Mo JH, Lee CH, Rhee CS, Kim JW (October 2009). "Treatment of postviral olfactory loss with glucocorticoids, Ginkgo biloba, and mometasone nasal spray". Archives of Otolaryngology–Head & Neck Surgery. 135 (10): 1000–4. doi:10.1001/archoto.2009.141. PMID 19841338. Lay summary – ScienceDaily (October 19, 2009).
- Rupp, Claudia I.; Fleischhacker, W. Wolfgang; Kemmler, Georg; Kremser, Christian; Bilder, Robert M.; Mechtcheriakov, Sergei; Szeszko, Philip R.; Walch, Thomas; Scholtz, Arne W.; Klimbacher, Martina; Maier, Claudia; Albrecht, Gudrun; Lechner-Schoner, Theresia; Felber, Stefan; Hinterhuber, Hartmann (2005). "Olfactory functions and volumetric measures of orbitofrontal and limbic regions in schizophrenia". Schizophrenia Research. 74 (2–3): 149–61. doi:10.1016/j.schres.2004.07.010. PMID 15721995.
- Kieff, D; Boey, H; Schaefer, P; Goodman, M; Joseph, M (1997). "Isolated neurosarcoidosis presenting as anosmia and visual changes". Otolaryngology–Head and Neck Surgery. 117 (6): S183–6. doi:10.1016/S0194-5998(97)70097-4. PMID 9419143.
- Harris, Gardiner (June 16, 2009). "F.D.A. Warns Against Use of Popular Cold Remedy". New York Times.
- Wheeler, TT; Alberts, MA; Dolan, TA; McGorray, SP (1995). "Dental, visual, auditory and olfactory complications in Paget's disease of bone". Journal of the American Geriatrics Society. 43 (12): 1384–91. doi:10.1111/j.1532-5415.1995.tb06618.x. PMID 7490390.
- Eriksen KD, Bøge-Rasmussen T, Kruse-Larsen C (June 1990). "Anosmia following operation for cerebral aneurysms in the anterior circulation". Journal of Neurosurgery. 72 (6): 864–5. doi:10.3171/jns.1990.72.6.0864. PMID 2338570.
- Leon-Sarmiento FE, Bayona EA, Bayona-Prieto J, Osman A, Doty RL (2012). "Profound olfactory dysfunction in myasthenia gravis". PLOS ONE. 7 (10): e45544. Bibcode:2012PLoSO...745544L. doi:10.1371/journal.pone.0045544. PMC 3474814. PMID 23082113.
- Anosmia Foundation (causes section)
- Churchman, Andrew; O’Leary, Margaret A; Buckley, Nicholas A; Page, Colin B; Tankel, Alan; Gavaghan, Chris; Holdgate, Anna; Brown, Simon G A; Isbister, Geoffrey K (December 2010). "Clinical effects of red-bellied black snake (Pseudechis porphyriacus) envenoming and correlation with venom concentrations: Australian Snakebite Project (ASP-11)". The Medical Journal of Australia. 193 (11): 696–700. PMID 21143062.
- "Anosmia / Loss Of Smell".
- Holbrook, Eric H.; Leopold, Donald A. (2003). "Anosmia: Diagnosis and management". Current Opinion in Otolaryngology & Head and Neck Surgery. 11 (1): 54–60. doi:10.1097/00020840-200302000-00012. PMID 14515104.
- Vowles RH, Bleach NR, Rowe-Jones JM (August 1997). "Congenital anosmia". International Journal of Pediatric Otorhinolaryngology. 41 (2): 207–14. doi:10.1016/S0165-5876(97)00075-X. PMID 9306177.
- Sumner, D (1971). "Appetite and Anosmia". The Lancet. 297 (7706): 970. doi:10.1016/S0140-6736(71)91470-X.
- Turnley W. M. H. (1963). "Anosmia". The Laryngoscope. 73 (4): 468–473. doi:10.1288/00005537-196304000-00012. PMID 13994924.
- McClay, John E (May 1, 2014). "Nasal Polyps Treatment & Management". Medscape.
- McIntyre JC, Davis EE, Joiner A, et al. (September 2012). "Gene therapy rescues cilia defects and restores olfactory function in a mammalian ciliopathy model". Nature Medicine. 18 (9): 1423–8. doi:10.1038/nm.2860. PMC 3645984. PMID 22941275.
- Gallagher, James (September 3, 2012). "Gene therapy restores sense of smell in mice". BBC News.
Further reading
- Blodgett, Bonnie (2010). Remembering Smell: A Memoir of Losing—and Discovering—the Primal Sense. Houghton Mifflin Harcourt. ISBN 978-0-618-86188-0.
- Birnbaum, Molly (2011). Season to Taste: How I Lost my Sense of Smell and Found my Way. Ecco. ISBN 0-06-191531-9
- DeVere, Ronald & Calvert, Marjorie (2010). Navigating Smell and Taste Disorders. Demos Health. ISBN 978-1-932603-96-5
- Gilbert, Avery (2008). What the Nose Knows.The Science of Scent in Everyday Life. Crown. ISBN 978-1-4000-8234-6
- Herz, Rachel (2007). The Scent of Desire. Discovering Our Enigmatic Sense of Smell. HarperCollins. ISBN 978-0-06-082538-6
- Tafalla, Marta (2010). Nunca sabrás a qué huele Bagdad (You will never know the smell of Bagdad) (in Spanish). Autonomous University of Barcelona. ISBN 978-84-490-2611-9. - Novel dealing with congenital anosmia.
- Keller A, Malaspina D (2013). "Hidden consequences of olfactory dysfunction: a patient report series". BMC Ear, Nose and Throat Disorders. 13 (1): 8. doi:10.1186/1472-6815-13-8. PMC 3733708. PMID 23875929.
- Tafalla M (September 2013). "A world without the olfactory dimension". Anatomical Record. 296 (9): 1287–96. doi:10.1002/ar.22734. PMID 23907763.
- Tafalla, Marta (2013). "Anosmic Aesthetics", in: Estetika. The Central European Journal of Aesthetics, Prag, issue 1/2013, pp 53–80.
- Wilson, Donald A. & Stevenson, Richard J. (2006). Learning to Smell. Olfactory Perception from Neurobiology to Behavior. The Johns Hopkins University Press. ISBN 978-0-8018-8368-2