Locus coeruleus
The locus coeruleus (\-si-ˈrü-lē-əs\, also spelled locus caeruleus or locus ceruleus[1]) is a nucleus in the pons of the brainstem involved with physiological responses to stress and panic. It is a part of the reticular activating system.
| Locus coeruleus | |
|---|---|
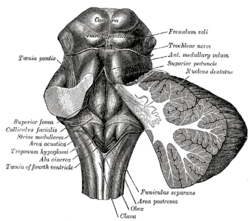 Rhomboid fossa. (Locus coeruleus not labeled, but is very near [just lateral to] the colliculus facialis, which is labeled at center left.) | |
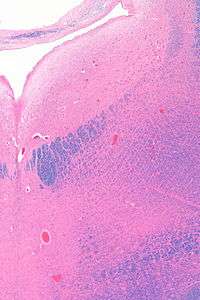
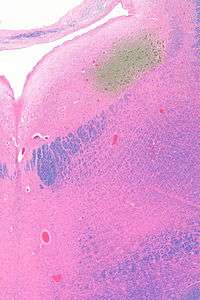
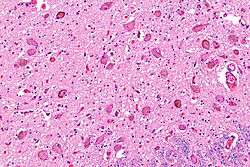 Micrograph showing the locus coeruleus. HE-LFB stain. | |
| Details | |
| Identifiers | |
| Latin | locus caeruleus ("blue place") |
| MeSH | D008125 |
| NeuroNames | 583 |
| NeuroLex ID | birnlex_905 |
| TA | A14.1.05.436 A14.1.05.706 |
| FMA | 72478 |
| Anatomical terms of neuroanatomy | |
The locus coeruleus is the principal site for brain synthesis of norepinephrine (noradrenaline). The locus coeruleus and the areas of the body affected by the norepinephrine it produces are described collectively as the locus coeruleus-noradrenergic system or LC-NA system.[2] Norepinephrine may also be released directly into the blood from the adrenal medulla.
Anatomy
The locus coeruleus (LC) is located in the posterior area of the rostral pons in the lateral floor of the fourth ventricle. It is composed of mostly medium-size neurons. Melanin granules inside the neurons of the LC contribute to its blue colour. Thus, it is also known as the nucleus pigmentosus pontis, meaning "heavily pigmented nucleus of the pons." The neuromelanin is formed by the polymerization of noradrenaline and is analogous to the black dopamine-based neuromelanin in the substantia nigra.
In adult humans (19-78) the locus coeruleus has 22,000 to 51,000 total pigmented neurons that range in size between 31,000 and 60,000 μm3.[3]
Connections
The projections of this nucleus reach far and wide. For example, they innervate the spinal cord, the brain stem, cerebellum, hypothalamus, the thalamic relay nuclei, the amygdala, the basal telencephalon, and the cortex. The norepinephrine from the LC has an excitatory effect on most of the brain, mediating arousal and priming the brain's neurons to be activated by stimuli.
As an important homeostatic control center of the body, the locus coeruleus receives afferents from the hypothalamus. The cingulate gyrus and the amygdala also innervate the LC, allowing emotional pain and stressors to trigger noradrenergic responses. The cerebellum and afferents from the raphe nuclei also project to the LC, in particular the pontine raphe nucleus and dorsal raphe nucleus.
Inputs
The locus coeruleus receives inputs from a number of other brain regions, primarily:
- The Medial prefrontal cortex, whose connection is constant, excitatory, and increases in strength with raised activity levels in the subject
- The Nucleus paragigantocellularis, which integrates autonomic and environmental stimuli
- The Nucleus prepositus, which is involved in gaze
- The Lateral hypothalamus, which releases orexin, which, as well as its other functions, is excitatory in the locus coeruleus.
Outputs
The projections from the locus coeruleus consist of neurons that utilize norepinephrine as their primary neurotransmitter.[4][5] These projections include the following connections:[4][5]
- LC → Amygdala and Hippocampus
- LC → Brain stem and Spinal cord
- LC → Cerebellum
- LC → Cerebral cortex
- LC → Hypothalamus
- LC → Tectum
- LC → Thalamus
- LC → Ventral tegmental area
Function
It is related to many functions via its widespread projections. The LC-NA system modulates cortical, subcortical, cerebellar, brainstem, and spinal cord circuits. Some of the most important functions influenced by this system are:[6][7]
- Arousal and sleep-wake cycle
- Attention and memory
- Behavioral flexibility, behavioral inhibition and stress (psychological)
- Cognitive control
- Emotions
- Neuroplasticity
- Posture and balance
The locus coeruleus is a part of the reticular activating system, and is almost completely inactivated in rapid eye movement sleep.[8]
Pathophysiology
The locus coeruleus may figure in clinical depression, panic disorder, Parkinson's disease, Alzheimer's disease[9] and anxiety. Some medications including norepinephrine reuptake inhibitors (reboxetine, atomoxetine), serotonin-norepinephrine reuptake inhibitors (venlafaxine, duloxetine), and norepinephrine-dopamine reuptake inhibitors (bupropion) are believed to show efficacy by acting upon neurons in this area.
Research continues to reveal that norepinephrine (NE) is a critical regulator of numerous activities from stress response, the formation of memory to attention and arousal. Many neuropsychiatric disorders precipitate from alterations to NE modulated neurocircuitry: disorders of affect, anxiety disorders, PTSD, ADHD and Alzheimer's disease. Alterations in the locus coeruleus (LC) accompany dysregulation of NE function and likely play a key role in the pathophysiology of these neuropsychiatric disorders.[10]
In stress
The locus coeruleus is responsible for mediating many of the sympathetic effects during stress. The locus coeruleus is activated by stress, and will respond by increasing norepinephrine secretion, which in turn will alter cognitive function (through the prefrontal cortex), increase motivation (through nucleus accumbens), activate the hypothalamic-pituitary-adrenal axis, and increase the sympathetic discharge/inhibit parasympathetic tone (through the brainstem). Specific to the activation of the hypothalamic-pituitary adrenal axis, norepinephrine will stimulate the secretion of corticotropin-releasing factor from the hypothalamus, that induces adrenocorticotropic hormone release from the anterior pituitary and subsequent cortisol synthesis in the adrenal glands. Norepinephrine released from locus coeruleus will feedback to inhibit its production, and corticotropin-releasing factor will feedback to inhibit its production, while positively feeding to the locus coeruleus to increase norepinephrine production.[11]
The LC's role in cognitive function in relation to stress is complex and multi-modal. Norepinephrine released from the LC can act on α2 receptors to increase working memory, or an excess of NE may decrease working memory by binding to the lower-affinity α1 receptors.[12]
Psychiatric research has documented that enhanced noradrenergic postsynaptic responsiveness in the neuronal pathway (brain circuit) that originates in the locus coeruleus and ends in the basolateral nucleus of the amygdala is a major factor in the pathophysiology of most stress-induced fear-circuitry disorders and especially in posttraumatic stress disorder (PTSD). The LC neurons are probably the origin of the first or second "leg" of the "PTSD circuit." An important 2005 study of deceased American army veterans from World War II has shown combat-related PTSD to be associated with a postmortem-diminished number of neurons in the locus coeruleus (LC) on the right side of the brain.[13]
In opiate withdrawal
Opioids inhibit the firing of neurons in the locus coeruleus. When opioid consumption is stopped, the increased activity of the locus coeruleus contributes to the symptoms of opiate withdrawal. The alpha2 adrenoceptor agonist clonidine is used to counteract this withdrawal effect by decreasing adrenergic neurotransmission from the locus coeruleus.[14]
Rett syndrome
The genetic defect of the transcriptional regulator MECP2 is responsible for Rett syndrome.[15] A MECP2 deficiency has been associated to catecholaminergic dysfunctions related to autonomic and sympathoadrenergic system in mouse models of Rett Syndrome (RTT). The locus coeruleus is the major source of noradrenergic innervation in the brain and sends widespread connections to rostral (cerebral cortex, hippocampus, hypothalamus) and caudal (cerebellum, brainstem nuclei) brain areas[16] and.[17] Indeed, an alteration of this structure could contribute to several symptoms observed in MECP2-deficient mice. Changes in the electrophysiological properties of cells in the locus ceruleus were shown. These Locus Coeruleus cell changes include hyperexcitability and decreased functioning of its noradrenergic innervation.[18] A reduction of the tyrosine hydroxylase (TH) mRNA level, the rate-limiting enzyme in catecholamine synthesis, was detected in the whole pons of MECP2-null male as well as in adult heterozygous female mice. Using immunoquantification techniques, a decrease of TH protein staining level, number of locus coeruleus TH-expressing neurons and density of dendritic arborization surrounding the structure was shown in symptomatic MECP2-deficient mice.[19] However, locus coeruleus cells are not dying but are more likely losing their fully mature phenotype, since no apoptotic neurons in the pons were detected.[19] Researchers have concluded that, "Because these neurons are a pivotal source of norepinephrine throughout the brainstem and forebrain and are involved in the regulation of diverse functions disrupted in Rett Syndrome, such as respiration and cognition, we hypothesize that the locus ceruleus is a critical site at which loss of MECP2 results in CNS dysfunction. Restoration of normal locus ceruleus function may therefore be of potential therapeutic value in the treatment of Rett Syndrome."[18] This could explain why a norepinephrine reuptake inhibitor (desipramine, DMI), which enhances the extracellular NE levels at all noradrenergic synapses, ameliorated some Rett syndrome symptoms in a mouse model of Rett syndrome.[19]
Neurodegenerative diseases
The locus ceruleus is affected in many forms of neurodegenerative diseases: genetic and idiopathic Parkinson's disease, progressive supranuclear palsy, Pick's disease or Alzheimer's disease. It is also affected in Down syndrome.[20] For example, there is up to 80% loss of locus ceruleus neurons in Alzheimer's disease.[21] Mouse models of Alzheimer's disease show accelerated progression after chemical destruction of the locus ceruleus[22] The norepinephrine from locus ceruleus cells in addition to its neurotransmitter role locally diffuses from "varicosities". As such it provides an endogenous anti-inflammatory agent in the microenvironment around the neurons, glial cells, and blood vessels in the neocortex and hippocampus.[9] It has been shown that norepinephrine stimulates mouse microglia to suppress Aβ-induced production of cytokines and promotes phagocytosis of Aβ.[9] This suggests that degeneration of the locus ceruleus might be responsible for increased Aβ deposition in AD brains.[9] Degeneration of pigmented neurons in this region in Alzheimer's and Parkinson's disease can be visualized in vivo with Neuromelanin MRI.[23]
History
It was discovered in 1784 by Félix Vicq-d'Azyr,[24] redescribed later by Johann Christian Reil in 1809[25] and named by Joseph Wenzel and Karl Wenzel brothers in 1812.[26][27] High monoamine oxidase activity in the rodent LC was found in 1959, monoamines were found in 1964 and noradrenergic ubiquitous projections in the 1970s.[25]
Etymology
Coeruleus or caeruleus
The 'English' name locus coeruleus[28] is actually a Latin expression consisting of the noun, locus, place or spot[29] and the adjective coeruleus, dark blue[29] or sky-blue.[30][31] This was aptly translated into English as blue place in 1907 in the English translation[32] of the official Latin anatomic nomenclature of 1895, Nomina Anatomica. The name of the locus coeruleus is derived from its azure appearance in unstained brain tissue.[26] The color is due to light scattering from neuromelanin in noradrenergic (producing or activated by norepinephrine) nerve cell bodies. The phenomenon is magnified by the Falck-Hillarp technique, which combines freeze-dried tissue and formaldehyde to fluoresce the catecholamines and serotonin contained in the tissue.
The spelling coeruleus is actually considered incorrect[33] with dictionaries of classical Latin preferring caeruleus[29][34] instead. Caeruleus is derived from caelum,[34] hence the spelling with -ae, like caeluleus → caeruleus.[34] Caelum in classical Latin could refer to the sky, the heaven or the vault of heaven.[29]
In mediaeval Latin, orthographic variants like coelum[35] for classical Latin caelum[29] and cerulans[35] for classical Latin caerulans[29] can be spotted.
In English, the color adjective cerulean is derived from Latin caeruleus.[36] In addition, ceiling is ultimately derived from Latin caelum as well.[37]
Official Latin nomenclature
The official Latin nomenclature, Nomina Anatomica as ratified in Basel in 1895[38] and in Jena in 1935[39][40] contained the orthographic correct form locus caeruleus. The Nomina Anatomica published in 1955[41] inadvertently introduced the incorrect spelling locus coeruleus, without any further explanation. The subsequent edition monophthongized the diphthong, resulting in locus ceruleus,[42] as they proclaimed that: "All diphthongs should be eliminated".[43] This form was retained in the subsequent edition.[43] The following two editions from 1977[44] and 1983[45] reverted the orthography back to the incorrect spelling locus coeruleus, while the subsequent edition from 1989[46] eventually returned to the correct spelling locus caeruleus. The current edition of the Nomina Anatomica, rebaptized as Terminologia Anatomica,[47] dictates locus caeruleus in its list of Latin expressions and correspondingly mentions locus caeruleus in its list of English equivalents. This is in line with the statement made by the chairman of the Terminologia Anatomica that "the committee decided that Latin terms when used in English should be in correct Latin".[48]
See also
References
- "locus coeruleus | a bluish area of the brain stem with many norepinephrine-containing neurons". www.merriam-webster.com. Retrieved 26 July 2015.
- Mehler, Mark F.; Dominick P. Purpura (March 2009). "Autism, fever, epigenetics and the locus coeruleus". Brain Research Reviews. 59 (2): 388–392. doi:10.1016/j.brainresrev.2008.11.001. PMC 2668953. PMID 19059284.
- Mouton PR, Pakkenberg B, Gundersen HJ, Price DL (August 1994). "Absolute number and size of pigmented locus coeruleus neurons in young and aged individuals". J. Chem. Neuroanat. 7 (3): 185–90. doi:10.1016/0891-0618(94)90028-0. PMID 7848573.
- Malenka RC, Nestler EJ, Hyman SE (2009). "Chapter 6: Widely Projecting Systems: Monoamines, Acetylcholine, and Orexin". In Sydor A, Brown RY (eds.). Molecular Neuropharmacology: A Foundation for Clinical Neuroscience (2nd ed.). New York: McGraw-Hill Medical. p. 155. ISBN 9780071481274.
Different subregions of the VTA receive glutamatergic inputs from the prefrontal cortex, orexinergic inputs from the lateral hypothalamus, cholinergic and also glutamatergic and GABAergic inputs from the laterodorsal tegmental nucleus and pedunculopontine nucleus, noradrenergic inputs from the locus ceruleus, serotonergic inputs from the raphe nuclei, and GABAergic inputs from the nucleus accumbens and ventral pallidum.
- Malenka RC, Nestler EJ, Hyman SE (2009). "Chapter 6: Widely Projecting Systems: Monoamines, Acetylcholine, and Orexin". In Sydor A, Brown RY (eds.). Molecular Neuropharmacology: A Foundation for Clinical Neuroscience (2nd ed.). New York: McGraw-Hill Medical. pp. 156–157. ISBN 9780071481274.
The locus ceruleus (LC), which is located on the floor of the fourth ventricle in the rostral pons, contains more than 50% of all noradrenergic neurons in the brain; it innervates both the forebrain (eg, it provides virtually all the NE to the cerebral cortex) and regions of the brainstem and spinal cord. ... The other noradrenergic neurons in the brain occur in loose collections of cells in the brainstem, including the lateral tegmental regions. These neurons project largely within the brainstem and spinal cord. NE, along with 5HT, ACh, histamine, and orexin, is a critical regulator of the sleep-wake cycle and of levels of arousal. ... LC firing may also increase anxiety ...Stimulation of β-adrenergic receptors in the amygdala results in enhanced memory for stimuli encoded under strong negative emotion ... Epinephrine occurs in only a small number of central neurons, all located in the medulla. Epinephrine is involved in visceral functions, such as control of respiration.
- Benarroch EE (November 2009). "The locus ceruleus norepinephrine system: functional organization and potential clinical significance". Neurology. 73 (20): 1699–704. doi:10.1212/WNL.0b013e3181c2937c. PMID 19917994.
- Malenka RC, Nestler EJ, Hyman SE (2009). "Chapter 6: Widely Projecting Systems: Monoamines, Acetylcholine, and Orexin". In Sydor A, Brown RY (eds.). Molecular Neuropharmacology: A Foundation for Clinical Neuroscience (2nd ed.). New York: McGraw-Hill Medical. p. 157. ISBN 9780071481274.
- Schwartz, JR; Roth, T (December 2008). "Neurophysiology of sleep and wakefulness: basic science and clinical implications". Current Neuropharmacology. 6 (4): 367–78. doi:10.2174/157015908787386050. PMC 2701283. PMID 19587857.
- Heneka MT, Nadrigny F, Regen T, Martinez-Hernandez A, Dumitrescu-Ozimek L, Terwel D, Jardanhazi-Kurutz D, Walter J, Kirchhoff F, Hanisch UK, Kummer MP (2010). "Locus ceruleus controls Alzheimer's disease pathology by modulating microglial functions through norepinephrine". Proc Natl Acad Sci U S A. 107 (13): 6058–6063. doi:10.1073/pnas.0909586107. PMC 2851853. PMID 20231476.
- Ressler KJ, Nemeroff CB. Role of norepinephrine in the pathophysiology of neuropsychiatric disorders. CNS Spectr. 2001 Aug;6(8):663-6, 670.
- Benarroch EE (November 2009). "The locus coeruleus norepinephrine system: functional organization and potential clinical significance". Neurology. 73 (20): 1699–704. doi:10.1212/wnl.0b013e3181c2937c. PMID 19917994.
- Ramos BP, Arnsten AF (2007). "Adrenergic pharmacology and cognition: focus on the prefrontal cortex". Pharmacol Ther. 113 (3): 523–536. doi:10.1016/j.pharmthera.2006.11.006. PMC 2151919. PMID 17303246.
- Bracha HS, Garcia-Rill E, Mrak RE, Skinner R (2005). "Postmortem locus coeruleus neuron count in three American veterans with probable or possible war-related PTSD". The Journal of Neuropsychiatry and Clinical Neurosciences. 17 (4): 503–9. doi:10.1176/appi.neuropsych.17.4.503. PMC 4484762. PMID 16387990.
- Devenyi P.; Mitwalli A.; Graham W. (November 1982). "Clonidine therapy for narcotic withdrawal". Can Med Assoc J. 127 (10): 1009–1011. PMC 1862300. PMID 7139433.
- Amir RE, Van, den Veyver IB, Wan M, Tran CQ, Francke U, Zoghbi HY (October 1999). "Rett Syndrome is caused by mutations in X-linked MECP2, encoding methyl-CpG-binding protein 2". Nat Genet. 23 (2): 185–8. doi:10.1038/13810. PMID 10508514.CS1 maint: multiple names: authors list (link)
- Hokfelt T, Martensson R, Bjorklund A, Kleinau S, Goldstein M. 1984. Distribution maps of tyrosine-hydroxylase-immunoreactive neurons in the rat brain. In Handbook of Chemical Neuroanatomy, Vol. 2. Classical Transmitters in the CNS, Part I ( A. Bjorklund and T. Hokfelt, eds.) pp. 277-379. Elsevier, New York.
- Berridge CW, Waterhouse BD (2003). "The locus coeruleus-noradrenergic system: modulation of behavioral state and state-dependent cognitive processes". Brain Res Rev. 42 (1): 33–84. doi:10.1016/s0165-0173(03)00143-7. PMID 12668290.
- Taneja P, Ogier M, Brooks-Harris G, Schmid DA, Katz DM, Nelson SB (2009). "Pathophysiology of Locus Ceruleus Neurons in a Mouse Model of Rett Syndrome". Journal of Neuroscience. 29 (39): 12187–12195. doi:10.1523/JNEUROSCI.3156-09.2009. PMC 2846656. PMID 19793977.
- Roux JC, Panayotis N, Dura E, Villard L (2009). "Progressive Noradrenergic Deficits in the Locus Coeruleus of MECP2 Deficient Mice". J Neurosci Res. 88 (7): 1500–9. doi:10.1002/jnr.22312. PMID 19998492. Archived from the original on 18 December 2012.
- Esiri MM. et al. (2004). Neuropathology of dementia. 2nd ed. Cambridge University Press.
- Bondareff W, Mountjoy CQ, Roth M (February 1982). "Loss of neurons of origin of the adrenergic projection to cerebral cortex (nucleus locus ceruleus) in senile dementia". Neurology. 32 (2): 164–8. doi:10.1212/wnl.32.2.164. PMID 7198741.
- Heneka MT, Ramanathan M, Jacobs AH, Dumitrescu-Ozimek L, Bilkei-Gorzo A, Debeir T, Sastre M, Galldiks N, Zimmer A, Hoehn M, Heiss WD, Klockgether T, Staufenbiel M (February 2006). "Locus ceruleus degeneration promotes Alzheimer pathogenesis in amyloid precursor protein 23 transgenic mice". J Neurosci. 26 (5): 1343–54. doi:10.1523/jneurosci.4236-05.2006. PMC 6675491. PMID 16452658.
- Sasaki M, Shibata E, Tohyama K, Takahashi J, Otsuka K, Tsuchiya K, Takahashi S, Ehara S, Terayama Y, Sakai A (July 2006). "Neuromelanin magnetic resonance imaging of locus ceruleus and substantia nigra in Parkinson's disease". NeuroReport. 17 (11): 1215–8. doi:10.1097/01.wnr.0000227984.84927.a7. PMID 16837857.
- Tubbs RS, Loukas M, Shoja MM, Mortazavi MM, Cohen-Gadol AA (July 2011). "Félix Vicq d'Azyr (1746-1794): early founder of neuroanatomy and royal French physician". Childs Nerv Syst. 27 (7): 1031–4. doi:10.1007/s00381-011-1424-y. PMID 21445631.
- Maeda T (February 2000). "The locus coeruleus: history". J. Chem. Neuroanat. 18 (1–2): 57–64. doi:10.1016/s0891-0618(99)00051-4. PMID 10708919.
- Wenzel, Josephus; Wenzel, Carolus (1812). De penitiori structura cerebri hominis et brutorum (in Latin). Tübingen: Cottam. p. 168. Retrieved 26 July 2019.
- Swanson, LW. Neuroanatomical terminology : a lexicon of classical origins and historical foundations. Oxford University Press, 2014. England ISBN 9780195340624
- Anderson, D.M. (2000). Dorland's illustrated medical dictionary (29th edition). Philadelphia/London/Toronto/Montreal/Sydney/Tokyo: W.B. Saunders Company.
- Lewis, C.T. & Short, C. (1879). A Latin dictionary founded on Andrews' edition of Freund's Latin dictionary. Oxford: Clarendon Press.
- Kraus, L.A. (1844). Kritisch-etymologisches medicinisches Lexikon (Dritte Auflage). Göttingen: Verlag der Deuerlich- und Dieterichschen Buchhandlung.
- Foster, F.D. (1891-1893). An illustrated medical dictionary. Being a dictionary of the technical terms used by writers on medicine and the collateral sciences, in the Latin, English, French, and German languages. New York: D. Appleton and Company.
- Barker, L.W. (1907). Anatomical terminology with special reference to the [BNA]. With vocabularies in Latin and English and illustrations. Philadelphia: P. Blakiston's Son & Co.
- Triepel, H. (1910). Die anatomischen Namen. Ihre Ableitung und Aussprache. Mit einem Anhang: Biographische Notizen.(Dritte Auflage). Wiesbaden: Verlag J.F. Bergmann.
- Wageningen, J. van & Muller, F. (1921). Latijnsch woordenboek. (3de druk). Groningen/Den Haag: J.B. Wolters' Uitgevers-Maatschappij
- Niermeyer, J.F. (1976). Mediae Latinitatis lexicon minus.Lexique Latin médiéval-Français/Anglais. A medieval Latin-French/English dictionary. Leiden: E.J. BriLL.
- Donald, J. (1880). Chambers's etymological dictionary of the English language. London/Edinburgh: W. & R. Chambers.
- Klein, E. (1971). A comprehensive etymological dictionary of the English language. Dealing with the origin of words and their sense development thus illustration the history of civilization and culture. Amsterdam: Elsevier Science B.V.
- His, W. (1895). Die anatomische Nomenclatur. Nomina Anatomica. Der von der Anatomischen Gesellschaft auf ihrer IX. Versammlung in Basel angenommenen Namen. Leipzig: Verlag Veit & Comp.
- Kopsch, F. (1941). Die Nomina anatomica des Jahres 1895 (B.N.A.) nach der Buchstabenreihe geordnet und gegenübergestellt den Nomina anatomica des Jahres 1935 (I.N.A.) (3. Auflage). Leipzig: Georg Thieme Verlag.
- Stieve, H. (1949). Nomina Anatomica. Zusammengestellt von der im Jahre 1923 gewählten Nomenklatur-Kommission, unter Berücksichtigung der Vorschläge der Mitglieder der Anatomischen Gesellschaft, der Anatomical Society of Great Britain and Ireland, sowie der American Association of Anatomists, überprüft und durch Beschluß der Anatomischen Gesellschaft auf der Tagung in Jena 1935 endgúltig angenommen. (4th edition). Jena: Verlag Gustav Fischer.
- International Anatomical Nomenclature Committee (1955). Nomina Anatomica . London/Colchester:Spottiswoode, Ballantyne and Co. Ltd.
- Donáth, T. & Crawford, G.C.N. (1969). Anatomical dictionary with nomenclature and explanatory notes. Oxford/London/Edinburgh/New York/Toronto/Syney/Paris/Braunschweig: Pergamon Press.
- International Anatomical Nomenclature Committee (1966). Nomina Anatomica. Amsterdam: Excerpta Medica Foundation.
- International Anatomical Nomenclature Committee (1977). Nomina Anatomica, together with Nomina Histologica and Nomina Embryologica. Amsterdam-Oxford: Excerpta Medica.
- International Anatomical Nomenclature Committee (1983). Nomina Anatomica, together with Nomina Histologica and Nomina Embryologica. Baltimore/London: Williams & Wilkins
- International Anatomical Nomenclature Committee (1989). Nomina Anatomica, together with Nomina Histologica and Nomina Embryologica. Edinburgh: Churchill Livingstone.
- Federative Committee on Anatomical Terminology (FCAT) (1998). Terminologia Anatomica. Stuttgart: Thieme
- Whitmore, I. (2009). "Terminologia Anatomica includes terms in English for all scientists writing in English". Anatomical Sciences Education. 2 (3): 141. doi:10.1002/ase.88. PMID 19496164.
A novel based upon real facts by Max Trasin, Pentian 2016
External links
| Wikimedia Commons has media related to Locus coeruleus. |
- "A Lecture, Higher Brain Function: Activation of the Brain and Levels of Consciousness" at East Tennessee State University
- Stained brain slice images which include the "locus coeruleus" at the BrainMaps project
- Diagram at University of Texas at Austin
- Diagram at University of Virginia
- https://web.archive.org/web/20070512234228/http://www2.umdnj.edu/~neuro/studyaid/Practical2000/Q45.htm
{kind=link}
| Authority control |
|---|