Leukemia
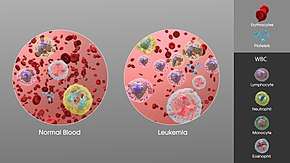
Leukemia, also spelled leukaemia, is a group of blood cancers that usually begin in the bone marrow and result in high numbers of abnormal blood cells.[8] These blood cells are not fully developed and are called blasts or leukemia cells.[2] Symptoms may include bleeding and bruising, feeling tired, fever, and an increased risk of infections.[2] These symptoms occur due to a lack of normal blood cells.[2] Diagnosis is typically made by blood tests or bone marrow biopsy.[2]
| Leukemia | |
|---|---|
| Other names | Leukaemia |
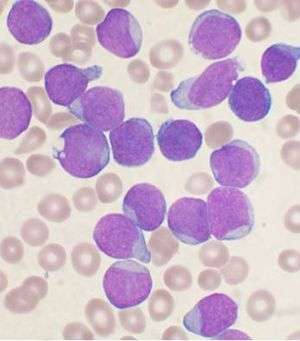 | |
| A Wright's stainled bone marrow aspirate smear from a person with precursor B-cell acute lymphoblastic leukemia. | |
| Pronunciation |
|
| Specialty | Hematology and oncology |
| Symptoms | Bleeding, bruising, feeling tired, fever, increased risk of infections[2] |
| Usual onset | All ages,[3] most common in 60s and 70s[4] |
| Causes | Inherited and environmental factors[5] |
| Risk factors | Smoking, family history, ionizing radiation, some chemicals, prior chemotherapy, Down syndrome.[3][5] |
| Diagnostic method | Blood tests, bone marrow biopsy[2] |
| Treatment | Chemotherapy, radiation therapy, targeted therapy, bone marrow transplant, supportive care[3] |
| Prognosis | Five-year survival rate 57% (USA)[4] |
| Frequency | 2.3 million (2015)[6] |
| Deaths | 353,500 (2015)[7] |
The exact cause of leukemia is unknown.[5] A combination of genetic factors and environmental (non-inherited) factors are believed to play a role.[5] Risk factors include smoking, ionizing radiation, some chemicals (such as benzene), prior chemotherapy, and Down syndrome.[5][3] People with a family history of leukemia are also at higher risk.[3] There are four main types of leukemia—acute lymphoblastic leukemia (ALL), acute myeloid leukemia (AML), chronic lymphocytic leukemia (CLL) and chronic myeloid leukemia (CML)—as well as a number of less common types.[3][9] Leukemias and lymphomas both belong to a broader group of tumors that affect the blood, bone marrow, and lymphoid system, known as tumors of the hematopoietic and lymphoid tissues.[10][11]
Treatment may involve some combination of chemotherapy, radiation therapy, targeted therapy, and bone marrow transplant, in addition to supportive care and palliative care as needed.[3] Certain types of leukemia may be managed with watchful waiting.[3] The success of treatment depends on the type of leukemia and the age of the person. Outcomes have improved in the developed world.[9] The average five-year survival rate is 57% in the United States.[4] In children under 15, the five-year survival rate is greater than 60 to 90%, depending on the type of leukemia.[12] In children with acute leukemia who are cancer-free after five years, the cancer is unlikely to return.[12]
In 2015, leukemia was present in 2.3 million people and caused 353,500 deaths.[6][7] In 2012 it newly developed in 352,000 people.[9] It is the most common type of cancer in children, with three quarters of leukemia cases in children being the acute lymphoblastic type.[3] However, over 90% of all leukemias are diagnosed in adults, with CLL and AML being most common in adults.[3] It occurs more commonly in the developed world.[9]
Classification
| Cell type | Acute | Chronic |
|---|---|---|
| Lymphocytic leukemia (or "lymphoblastic") | Acute lymphoblastic leukemia (ALL) | Chronic lymphocytic leukemia (CLL) |
| Myelogenous leukemia ("myeloid" or "nonlymphocytic") | Acute myelogenous leukemia (AML or myeloblastic) | Chronic myelogenous leukemia (CML) |
General classification
Clinically and pathologically, leukemia is subdivided into a variety of large groups. The first division is between its acute and chronic forms:
- Acute leukemia is characterized by a rapid increase in the number of immature blood cells. The crowding that results from such cells makes the bone marrow unable to produce healthy blood cells. Immediate treatment is required in acute leukemia because of the rapid progression and accumulation of the malignant cells, which then spill over into the bloodstream and spread to other organs of the body. Acute forms of leukemia are the most common forms of leukemia in children.
- Chronic leukemia is characterized by the excessive buildup of relatively mature, but still abnormal, white blood cells. Typically taking months or years to progress, the cells are produced at a much higher rate than normal, resulting in many abnormal white blood cells. Whereas acute leukemia must be treated immediately, chronic forms are sometimes monitored for some time before treatment to ensure maximum effectiveness of therapy. Chronic leukemia mostly occurs in older people, but can occur in any age group.
Additionally, the diseases are subdivided according to which kind of blood cell is affected. This divides leukemias into lymphoblastic or lymphocytic leukemias and myeloid or myelogenous leukemias:
- In lymphoblastic or lymphocytic leukemias, the cancerous change takes place in a type of marrow cell that normally goes on to form lymphocytes, which are infection-fighting immune system cells. Most lymphocytic leukemias involve a specific subtype of lymphocyte, the B cell.
- In myeloid or myelogenous leukemias, the cancerous change takes place in a type of marrow cell that normally goes on to form red blood cells, some other types of white cells, and platelets.
Combining these two classifications provides a total of four main categories. Within each of these main categories, there are typically several subcategories. Finally, some rarer types are usually considered to be outside of this classification scheme.
Specific types
- Acute lymphoblastic leukemia (ALL) is the most common type of leukemia in young children. It also affects adults, especially those 65 and older. Standard treatments involve chemotherapy and radiotherapy. Subtypes include precursor B acute lymphoblastic leukemia, precursor T acute lymphoblastic leukemia, Burkitt's leukemia, and acute biphenotypic leukemia. While most cases of ALL occur in children, 80% of deaths from ALL occur in adults.[13]
- Chronic lymphocytic leukemia (CLL) most often affects adults over the age of 55. It sometimes occurs in younger adults, but it almost never affects children. Two-thirds of affected people are men. The five-year survival rate is 85%.[14] It is incurable, but there are many effective treatments. One subtype is B-cell prolymphocytic leukemia, a more aggressive disease.
- Acute myelogenous leukemia (AML) occurs far more commonly in adults than in children, and more commonly in men than women. It is treated with chemotherapy. The five-year survival rate is 20%.[15] One subtype is APL (Acute Promyelocytic Leukemia), which has a survival rate greater than 90%.[16] Subtypes of AML include acute promyelocytic leukemia, acute myeloblastic leukemia, and acute megakaryoblastic leukemia.
- Chronic myelogenous leukemia (CML) occurs mainly in adults; a very small number of children also develop this disease. It is treated with imatinib (Gleevec in United States, Glivec in Europe) or other drugs.[17] The five-year survival rate is 90%.[18][19] One subtype is chronic myelomonocytic leukemia.
- Hairy cell leukemia (HCL) is sometimes considered a subset of chronic lymphocytic leukemia, but does not fit neatly into this category. About 80% of affected people are adult men. No cases in children have been reported. HCL is incurable but easily treatable. Survival is 96% to 100% at ten years.[20]
- T-cell prolymphocytic leukemia (T-PLL) is a very rare and aggressive leukemia affecting adults; somewhat more men than women are diagnosed with this disease.[21] Despite its overall rarity, it is the most common type of mature T cell leukemia;[22] nearly all other leukemias involve B cells. It is difficult to treat, and the median survival is measured in months.
- Large granular lymphocytic leukemia may involve either T-cells or NK cells; like hairy cell leukemia, which involves solely B cells, it is a rare and indolent (not aggressive) leukemia.[23]
- Adult T-cell leukemia is caused by human T-lymphotropic virus (HTLV), a virus similar to HIV. Like HIV, HTLV infects CD4+ T-cells and replicates within them; however, unlike HIV, it does not destroy them. Instead, HTLV "immortalizes" the infected T-cells, giving them the ability to proliferate abnormally. Human T-cell lymphotropic virus types I and II (HTLV-I/II) are endemic in certain areas of the world.
- Clonal eosinophilias (also called clonal hypereosinophilias) are a group of blood disorders characterized by the growth of eosinophils in the bone marrow, blood, and/or other tissues. They may be pre-cancerous or cancerous. Clonal eosinophilias involve a "clone" of eosinophils, i.e., a group of genetically identical eosinophils that all grew from the same mutated ancestor cell.[24] These disorders may evolve into chronic eosinophilic leukemia or may be associated with various forms of myeloid neoplasms, lymphoid neoplasms, myelofibrosis, or the myelodysplastic syndrome.[25][26][24]
Pre-leukemia
- Transient myeloproliferative disease, also termed transient leukemia, involves the abnormal proliferation of a clone of non-cancerous megakaryoblasts. The disease is restricted to individuals with Down syndrome or genetic changes similar to those in Down syndrome, develops in a baby during pregnancy or shortly after birth, and resolves within 3 months or, in ~10% of cases, progresses to acute megakaryoblastic leukemia. Transient myeloid leukemia is a pre-leukemic condition.[27][28][29]
Signs and symptoms
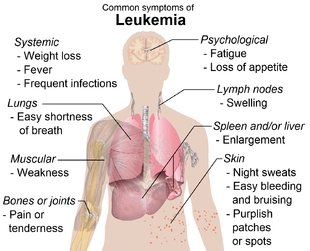
The most common symptoms in children are easy bruising, pale skin, fever, and an enlarged spleen or liver.[31]
Damage to the bone marrow, by way of displacing the normal bone marrow cells with higher numbers of immature white blood cells, results in a lack of blood platelets, which are important in the blood clotting process. This means people with leukemia may easily become bruised, bleed excessively, or develop pinprick bleeds (petechiae).
White blood cells, which are involved in fighting pathogens, may be suppressed or dysfunctional. This could cause the person's immune system to be unable to fight off a simple infection or to start attacking other body cells. Because leukemia prevents the immune system from working normally, some people experience frequent infection, ranging from infected tonsils, sores in the mouth, or diarrhea to life-threatening pneumonia or opportunistic infections.
Finally, the red blood cell deficiency leads to anemia, which may cause dyspnea and pallor.
Some people experience other symptoms, such as feeling sick, having fevers, chills, night sweats, feeling fatigued and other flu-like symptoms. Some people experience nausea or a feeling of fullness due to an enlarged liver and spleen; this can result in unintentional weight loss. Blasts affected by the disease may come together and become swollen in the liver or in the lymph nodes causing pain and leading to nausea.[32]
If the leukemic cells invade the central nervous system, then neurological symptoms (notably headaches) can occur. Uncommon neurological symptoms like migraines, seizures, or coma can occur as a result of brain stem pressure. All symptoms associated with leukemia can be attributed to other diseases. Consequently, leukemia is always diagnosed through medical tests.
The word leukemia, which means 'white blood', is derived from the characteristic high white blood cell count that presents in most afflicted people before treatment. The high number of white blood cells is apparent when a blood sample is viewed under a microscope, with the extra white blood cells frequently being immature or dysfunctional. The excessive number of cells can also interfere with the level of other cells, causing further harmful imbalance in the blood count.
Some people diagnosed with leukemia do not have high white blood cell counts visible during a regular blood count. This less-common condition is called aleukemia. The bone marrow still contains cancerous white blood cells which disrupt the normal production of blood cells, but they remain in the marrow instead of entering the bloodstream, where they would be visible in a blood test. For a person with aleukemia, the white blood cell counts in the bloodstream can be normal or low. Aleukemia can occur in any of the four major types of leukemia, and is particularly common in hairy cell leukemia.[33]
Causes
There is no single known cause for any of the different types of leukemias. The few known causes, which are not generally factors within the control of the average person, account for relatively few cases.[34] The cause for most cases of leukemia is unknown. The different leukemias likely have different causes.
Leukemia, like other cancers, results from mutations in the DNA. Certain mutations can trigger leukemia by activating oncogenes or deactivating tumor suppressor genes, and thereby disrupting the regulation of cell death, differentiation or division. These mutations may occur spontaneously or as a result of exposure to radiation or carcinogenic substances.[35]
Among adults, the known causes are natural and artificial ionizing radiation, a few viruses such as human T-lymphotropic virus, and some chemicals, notably benzene and alkylating chemotherapy agents for previous malignancies.[36][37][38] Use of tobacco is associated with a small increase in the risk of developing acute myeloid leukemia in adults.[36] Cohort and case-control studies have linked exposure to some petrochemicals and hair dyes to the development of some forms of leukemia. Diet has very limited or no effect, although eating more vegetables may confer a small protective benefit.[34]
Viruses have also been linked to some forms of leukemia. For example, human T-lymphotropic virus (HTLV-1) causes adult T-cell leukemia.[39]
A few cases of maternal-fetal transmission (a baby acquires leukemia because its mother had leukemia during the pregnancy) have been reported.[36] Children born to mothers who use fertility drugs to induce ovulation are more than twice as likely to develop leukemia during their childhoods than other children.[40]
Radiation
Large doses of Sr-90 emission from nuclear reactor accidents, nicknamed bone seeker increases the risk of bone cancer and leukemia in animals, and is presumed to do so in people.[41]
Genetic conditions
Some people have a genetic predisposition towards developing leukemia. This predisposition is demonstrated by family histories and twin studies.[36] The affected people may have a single gene or multiple genes in common. In some cases, families tend to develop the same kinds of leukemia as other members; in other families, affected people may develop different forms of leukemia or related blood cancers.[36]
In addition to these genetic issues, people with chromosomal abnormalities or certain other genetic conditions have a greater risk of leukemia.[37] For example, people with Down syndrome have a significantly increased risk of developing forms of acute leukemia (especially acute myeloid leukemia), and Fanconi anemia is a risk factor for developing acute myeloid leukemia.[36] Mutation in SPRED1 gene has been associated with a predisposition to childhood leukemia.[42]
Chronic myelogenous leukemia is associated with a genetic abnormality called the Philadelphia translocation; 95% of people with CML carry the Philadelphia mutation, although this is not exclusive to CML and can be observed in people with other types of leukemia.[43][44][45][46]
Non-ionizing radiation
Whether or not non-ionizing radiation causes leukemia has been studied for several decades. The International Agency for Research on Cancer expert working group undertook a detailed review of all data on static and extremely low frequency electromagnetic energy, which occurs naturally and in association with the generation, transmission, and use of electrical power.[47] They concluded that there is limited evidence that high levels of ELF magnetic (but not electric) fields might cause some cases of childhood leukemia.[47] No evidence for a relationship to leukemia or another form of malignancy in adults has been demonstrated.[47] Since exposure to such levels of ELFs is relatively uncommon, the World Health Organization concludes that ELF exposure, if later proven to be causative, would account for just 100 to 2400 cases worldwide each year, representing 0.2 to 4.9% of the total incidence of childhood leukemia for that year (about 0.03 to 0.9% of all leukemias).[48]
Diagnosis
Diagnosis is usually based on repeated complete blood counts and a bone marrow examination following observations of the symptoms. Sometimes, blood tests may not show that a person has leukemia, especially in the early stages of the disease or during remission. A lymph node biopsy can be performed to diagnose certain types of leukemia in certain situations.
Following diagnosis, blood chemistry tests can be used to determine the degree of liver and kidney damage or the effects of chemotherapy on the person. When concerns arise about other damages due to leukemia, doctors may use an X-ray, MRI, or ultrasound. These can potentially show leukemia's effects on such body parts as bones (X-ray), the brain (MRI), or the kidneys, spleen, and liver (ultrasound). CT scans can be used to check lymph nodes in the chest, though this is uncommon.
Despite the use of these methods to diagnose whether or not a person has leukemia, many people have not been diagnosed because many of the symptoms are vague, non-specific, and can refer to other diseases. For this reason, the American Cancer Society estimates that at least one-fifth of the people with leukemia have not yet been diagnosed.[33]
Treatment
Most forms of leukemia are treated with pharmaceutical medication, typically combined into a multi-drug chemotherapy regimen. Some are also treated with radiation therapy. In some cases, a bone marrow transplant is effective.
Acute lymphoblastic
Management of ALL is directed towards control of bone marrow and systemic (whole-body) disease. Additionally, treatment must prevent leukemic cells from spreading to other sites, particularly the central nervous system (CNS) e.g. monthly lumbar punctures. In general, ALL treatment is divided into several phases:
- Induction chemotherapy to bring about bone marrow remission. For adults, standard induction plans include prednisone, vincristine, and an anthracycline drug; other drug plans may include L-asparaginase or cyclophosphamide. For children with low-risk ALL, standard therapy usually consists of three drugs (prednisone, L-asparaginase, and vincristine) for the first month of treatment.
- Consolidation therapy or intensification therapy to eliminate any remaining leukemia cells. There are many different approaches to consolidation, but it is typically a high-dose, multi-drug treatment that is undertaken for a few months. People with low- to average-risk ALL receive therapy with antimetabolite drugs such as methotrexate and 6-mercaptopurine (6-MP). People who are high-risk receive higher drug doses of these drugs, plus additional drugs.
- CNS prophylaxis (preventive therapy) to stop the cancer from spreading to the brain and nervous system in high-risk people. Standard prophylaxis may include radiation of the head and/or drugs delivered directly into the spine.
- Maintenance treatments with chemotherapeutic drugs to prevent disease recurrence once remission has been achieved. Maintenance therapy usually involves lower drug doses, and may continue for up to three years.
- Alternatively, allogeneic bone marrow transplantation may be appropriate for high-risk or relapsed people.[49]
Chronic lymphocytic
Decision to treat
Hematologists base CLL treatment on both the stage and symptoms of the individual person. A large group of people with CLL have low-grade disease, which does not benefit from treatment. Individuals with CLL-related complications or more advanced disease often benefit from treatment. In general, the indications for treatment are:
- Falling hemoglobin or platelet count
- Progression to a later stage of disease
- Painful, disease-related overgrowth of lymph nodes or spleen
- An increase in the rate of lymphocyte production[50]
Treatment approach
For most people with CLL, it is incurable by present treatments, so treatment is directed towards suppressing the disease for many years, rather than totally and permanently eliminating it. The primary chemotherapeutic plan is combination chemotherapy with chlorambucil or cyclophosphamide, plus a corticosteroid such as prednisone or prednisolone. The use of a corticosteroid has the additional benefit of suppressing some related autoimmune diseases, such as immunohemolytic anemia or immune-mediated thrombocytopenia. In resistant cases, single-agent treatments with nucleoside drugs such as fludarabine,[51] pentostatin, or cladribine may be successful. Younger and healthier people may choose allogeneic or autologous bone marrow transplantation in the hope of a permanent cure.[52]
Acute myelogenous
Many different anti-cancer drugs are effective for the treatment of AML. Treatments vary somewhat according to the age of the person and according to the specific subtype of AML. Overall, the strategy is to control bone marrow and systemic (whole-body) disease, while offering specific treatment for the central nervous system (CNS), if involved.
In general, most oncologists rely on combinations of drugs for the initial, induction phase of chemotherapy. Such combination chemotherapy usually offers the benefits of early remission and a lower risk of disease resistance. Consolidation and maintenance treatments are intended to prevent disease recurrence. Consolidation treatment often entails a repetition of induction chemotherapy or the intensification chemotherapy with additional drugs. By contrast, maintenance treatment involves drug doses that are lower than those administered during the induction phase.[53]
Chronic myelogenous
There are many possible treatments for CML, but the standard of care for newly diagnosed people is imatinib (Gleevec) therapy.[54] Compared to most anti-cancer drugs, it has relatively few side effects and can be taken orally at home. With this drug, more than 90% of people will be able to keep the disease in check for at least five years,[54] so that CML becomes a chronic, manageable condition.
In a more advanced, uncontrolled state, when the person cannot tolerate imatinib, or if the person wishes to attempt a permanent cure, then an allogeneic bone marrow transplantation may be performed. This procedure involves high-dose chemotherapy and radiation followed by infusion of bone marrow from a compatible donor. Approximately 30% of people die from this procedure.[54]
Hairy cell
Decision to treat
People with hairy cell leukemia who are symptom-free typically do not receive immediate treatment. Treatment is generally considered necessary when the person shows signs and symptoms such as low blood cell counts (e.g., infection-fighting neutrophil count below 1.0 K/µL), frequent infections, unexplained bruises, anemia, or fatigue that is significant enough to disrupt the person's everyday life.
Typical treatment approach
People who need treatment usually receive either one week of cladribine, given daily by intravenous infusion or a simple injection under the skin, or six months of pentostatin, given every four weeks by intravenous infusion. In most cases, one round of treatment will produce a prolonged remission.[55]
Other treatments include rituximab infusion or self-injection with Interferon-alpha. In limited cases, the person may benefit from splenectomy (removal of the spleen). These treatments are not typically given as the first treatment because their success rates are lower than cladribine or pentostatin.[56]
T-cell prolymphocytic
Most people with T-cell prolymphocytic leukemia, a rare and aggressive leukemia with a median survival of less than one year, require immediate treatment.[57]
T-cell prolymphocytic leukemia is difficult to treat, and it does not respond to most available chemotherapeutic drugs.[57] Many different treatments have been attempted, with limited success in certain people: purine analogues (pentostatin, fludarabine, cladribine), chlorambucil, and various forms of combination chemotherapy (cyclophosphamide, doxorubicin, vincristine, prednisone CHOP, cyclophosphamide, vincristine, prednisone [COP], vincristine, doxorubicin, prednisone, etoposide, cyclophosphamide, bleomycin VAPEC-B). Alemtuzumab (Campath), a monoclonal antibody that attacks white blood cells, has been used in treatment with greater success than previous options.[57]
Some people who successfully respond to treatment also undergo stem cell transplantation to consolidate the response.[57]
Juvenile myelomonocytic
Treatment for juvenile myelomonocytic leukemia can include splenectomy, chemotherapy, and bone marrow transplantation.[58]
Prognosis
The success of treatment depends on the type of leukemia and the age of the person. Outcomes have improved in the developed world.[9] The average five-year survival rate is 61% in the United States.[4] In children under 15, the five-year survival rate is greater (60 to 85%), depending on the type of leukemia.[12] In children with acute leukemia who are cancer-free after five years, the cancer is unlikely to return.[12]
Outcomes depend on whether it is acute or chronic, the specific abnormal white blood cell type, the presence and severity of anemia or thrombocytopenia, the degree of tissue abnormality, the presence of metastasis and lymph node and bone marrow infiltration, the availability of therapies and the skills of the health care team. Treatment outcomes may be better when people are treated at larger centers with greater experience.[59]
Epidemiology
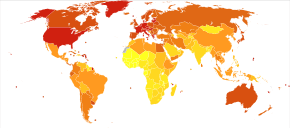
In 2010, globally, approximately 281,500 people died of leukemia.[60] In 2000, approximately 256,000 children and adults around the world developed a form of leukemia, and 209,000 died from it.[61] This represents about 3% of the almost seven million deaths due to cancer that year, and about 0.35% of all deaths from any cause.[61] Of the sixteen separate sites the body compared, leukemia was the 12th most common class of neoplastic disease, and the 11th most common cause of cancer-related death.[61] Leukemia occurs more commonly in the developed world.[62]
United States
About 245,000 people in the United States are affected with some form of leukemia, including those that have achieved remission or cure. Rates from 1975 to 2011 have increased by 0.7% per year among children.[63] Approximately 44,270 new cases of leukemia were diagnosed in the year 2008 in the US.[64] This represents 2.9% of all cancers (excluding simple basal cell and squamous cell skin cancers) in the United States, and 30.4% of all blood cancers.[65]
Among children with some form of cancer, about a third have a type of leukemia, most commonly acute lymphoblastic leukemia.[64] A type of leukemia is the second most common form of cancer in infants (under the age of 12 months) and the most common form of cancer in older children.[66] Boys are somewhat more likely to develop leukemia than girls, and white American children are almost twice as likely to develop leukemia than black American children.[66] Only about 3% cancer diagnoses among adults are for leukemias, but because cancer is much more common among adults, more than 90% of all leukemias are diagnosed in adults.[64]
Race is a risk factor in the United States. Hispanics, especially those under the age of 20, are at the highest risk for leukemia, while whites, Native Americans, Asian Americans, and Alaska Natives are at higher risk than African Americans.[67]
More men than women are diagnosed with leukemia and die from the disease. Around 30 percent more men than women have leukemia.[68]
UK
Overall, leukaemia is the eleventh most common cancer in the UK (around 8,600 people were diagnosed with the disease in 2011), and it is the ninth most common cause of cancer death (around 4,800 people died in 2012).[69]
History

Leukemia was first described by anatomist and surgeon Alfred-Armand-Louis-Marie Velpeau in 1827. A more complete description was given by pathologist Rudolf Virchow in 1845. Around ten years after Virchow's findings, pathologist Franz Ernst Christian Neumann found that the bone marrow of a deceased person with leukemia was colored "dirty green-yellow" as opposed to the normal red. This finding allowed Neumann to conclude that a bone marrow problem was responsible for the abnormal blood of people with leukemia.
By 1900 leukemia was viewed as a family of diseases as opposed to a single disease. By 1947 Boston pathologist Sidney Farber believed from past experiments that aminopterin, a folic acid mimic, could potentially cure leukemia in children. The majority of the children with ALL who were tested showed signs of improvement in their bone marrow, but none of them were actually cured. This, however, led to further experiments.
In 1962, researchers Emil J. Freireich, Jr. and Emil Frei III used combination chemotherapy to attempt to cure leukemia. The tests were successful with some people surviving long after the tests.[70]
Society and culture
According to Susan Sontag, leukemia was often romanticized in 20th-century fiction, portrayed as a joy-ending, clean disease whose fair, innocent and gentle victims die young or at the wrong time. As such, it was the cultural successor to tuberculosis, which held this cultural position until it was discovered to be an infectious disease.[72] The 1970 romance novel Love Story is an example of this romanticization of leukemia.
In the United States, around $5.4 billion is spent on treatment a year.[73]
Research directions
Significant research into the causes, prevalence, diagnosis, treatment, and prognosis of leukemia is being performed. Hundreds of clinical trials are being planned or conducted at any given time.[74] Studies may focus on effective means of treatment, better ways of treating the disease, improving the quality of life for people, or appropriate care in remission or after cures.
In general, there are two types of leukemia research: clinical or translational research and basic research. Clinical/translational research focuses on studying the disease in a defined and generally immediately applicable way, such as testing a new drug in people. By contrast, basic science research studies the disease process at a distance, such as seeing whether a suspected carcinogen can cause leukemic changes in isolated cells in the laboratory or how the DNA changes inside leukemia cells as the disease progresses. The results from basic research studies are generally less immediately useful to people with the disease.[75]
Treatment through gene therapy is currently being pursued. One such approach used genetically modified T cells, known as chimeric antigen receptor T cells (CAR-T cells), to attack cancer cells. In 2011, a year after treatment, two of the three people with advanced chronic lymphocytic leukemia were reported to be cancer-free[76] and in 2013, three of five subjects who had acute lymphocytic leukemia were reported to be in remission for five months to two years.[77] Subsequent studies with a variety of CAR-T types continue to be promising.[78] As of 2018, two CAR-T therapies have been approved by the Food and Drug Administration. CAR-T treatment has significant side effects,[79] and loss of the antigen targeted by the CAR-T cells is a common mechanism for relapse.[78] The stem cells that cause different types of leukaemia are also being researched.[80]
Pregnancy
Leukemia is rarely associated with pregnancy, affecting only about 1 in 10,000 pregnant women.[81] How it is handled depends primarily on the type of leukemia. Nearly all leukemias appearing in pregnant women are acute leukemias.[82] Acute leukemias normally require prompt, aggressive treatment, despite significant risks of pregnancy loss and birth defects, especially if chemotherapy is given during the developmentally sensitive first trimester.[81] Chronic myelogenous leukemia can be treated with relative safety at any time during pregnancy with Interferon-alpha hormones.[81] Treatment for chronic lymphocytic leukemias, which are rare in pregnant women, can often be postponed until after the end of the pregnancy.[81][82]
See also
- Acute erythroid leukemia
- Antileukemic drugs, medications used to kill leukemia cells
- Hematologic diseases, the large class of blood-related disorders, including leukemia
- Multiple myeloma
- Cancer-related fatigue
References
- "Leukemia". Merriam-Webster. Archived from the original on 6 October 2014.
- "What You Need To Know About™ Leukemia". National Cancer Institute. 23 December 2013. Archived from the original on 6 July 2014. Retrieved 18 June 2014.
- "A Snapshot of Leukemia". NCI. Archived from the original on 4 July 2014. Retrieved 18 June 2014.
- "SEER Stat Fact Sheets: Leukemia". National Cancer Institute. 2011. Archived from the original on 16 July 2016.
- Hutter, JJ (June 2010). "Childhood leukemia". Pediatrics in Review. 31 (6): 234–41. doi:10.1542/pir.31-6-234. PMID 20516235.
- GBD 2015 Disease and Injury Incidence and Prevalence, Collaborators. (8 October 2016). "Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015". Lancet. 388 (10053): 1545–1602. doi:10.1016/S0140-6736(16)31678-6. PMC 5055577. PMID 27733282.
- GBD 2015 Mortality and Causes of Death, Collaborators. (8 October 2016). "Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the Global Burden of Disease Study 2015". Lancet. 388 (10053): 1459–1544. doi:10.1016/s0140-6736(16)31012-1. PMC 5388903. PMID 27733281.
- "Leukemia". NCI. 1 January 1980. Archived from the original on 27 May 2014. Retrieved 13 June 2014.
Cancer that starts in blood-forming tissue, such as the bone marrow, and causes large numbers of abnormal blood cells
- World Cancer Report 2014. World Health Organization. 2014. pp. Chapter 5.13. ISBN 978-9283204299.
- Vardiman, JW; Thiele, J; Arber, DA; Brunning, RD; Borowitz, MJ; Porwit, A; Harris, NL; Le Beau, MM; Hellström-Lindberg, E; Tefferi, A; Bloomfield, CD (30 July 2009). "The 2008 revision of the World Health Organization (WHO) classification of myeloid neoplasms and acute leukemia: rationale and important changes". Blood. 114 (5): 937–51. doi:10.1182/blood-2009-03-209262. PMID 19357394.
- Cătoi, Alecsandru Ioan Baba, Cornel (2007). Comparative oncology. Bucharest: The Publishing House of the Romanian Academy. p. Chapter 17. ISBN 978-973-27-1457-7. Archived from the original on 10 September 2017.
- American Cancer Society (2 March 2014). "Survival rates for childhood leukemia". Archived from the original on 14 July 2014.
- "Key Statistics for Acute Lymphocytic Leukemia (ALL)". American Cancer Society. 8 January 2019. Retrieved 9 December 2019.
- Finding Cancer Statistics » Cancer Stat Fact Sheets »Chronic Lymphocytic Leukemia Archived 16 April 2008 at the Wayback Machine National Cancer Institute.
- "Survival: Acute Myeloid Leukaemia". Cancer Research UK. 10 July 2019. Retrieved 2 December 2019.
- Colvin G. A.; Elfenbein G. J. (2003). "The latest treatment advances for acute myelogenous leukemia". Medicine and Health, Rhode Island. 86 (8): 243–6. PMID 14582219.
- "Novartis Oncology". Archived from the original on 5 November 2013.
- Patients with Chronic Myelogenous Leukemia Continue to Do Well on Imatinib at 5-Year Follow-Up Archived 15 May 2013 at the Wayback Machine Medscape Medical News 2006.
- Updated Results of Tyrosine Kinase Inhibitors in CML Archived 29 December 2007 at the Wayback Machine ASCO 2006 Conference Summaries.
- Else, M., Ruchlemer, R., Osuji, N. (2005). "Long remissions in hairy cell leukemia with purine analogs: a report of 219 patients with a median follow-up of 12.5 years". Cancer. 104 (11): 2442–8. doi:10.1002/cncr.21447. PMID 16245328.CS1 maint: multiple names: authors list (link)
- Matutes Estella (1998). "T-cell prolymphocytic leukemia". Cancer Control. 5 (1): 19–24. doi:10.1177/107327489800500102. PMID 10761013. Archived from the original on 11 February 2009.
- Valbuena JR, Herling M, Admirand JH, Padula A, Jones D, Medeiros LJ (March 2005). "T-cell prolymphocytic leukemia involving extramedullary sites". American Journal of Clinical Pathology. 123 (3): 456–64. doi:10.1309/93P4-2RNG-5XBG-3KBE. PMID 15716243. Archived from the original on 15 May 2013.
- Elaine Sarkin Jaffe, Nancy Lee Harris, World Health Organization, International Agency for Research on Cancer, Harald Stein, J. W. Vardiman (2001). Pathology and genetics of tumours of haematopoietic and lymphoid tissues. World Health Organization Classification of Tumors. 3. Lyon: IARC Press. ISBN 978-92-832-2411-2.CS1 maint: multiple names: authors list (link)
- Reiter A, Gotlib J (2017). "Myeloid neoplasms with eosinophilia". Blood. 129 (6): 704–714. doi:10.1182/blood-2016-10-695973. PMID 28028030.
- Gotlib J (2015). "World Health Organization-defined eosinophilic disorders: 2015 update on diagnosis, risk stratification, and management". American Journal of Hematology. 90 (11): 1077–89. doi:10.1002/ajh.24196. PMID 26486351.
- Arber DA, Orazi A, Hasserjian R, Thiele J, Borowitz MJ, Le Beau MM, Bloomfield CD, Cazzola M, Vardiman JW (2016). "The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia". Blood. 127 (20): 2391–405. doi:10.1182/blood-2016-03-643544. PMID 27069254.
- Bhatnagar N, Nizery L, Tunstall O, Vyas P, Roberts I (October 2016). "Transient Abnormal Myelopoiesis and AML in Down Syndrome: an Update". Current Hematologic Malignancy Reports. 11 (5): 333–41. doi:10.1007/s11899-016-0338-x. PMC 5031718. PMID 27510823.
- Crispino JD, Horwitz MS (April 2017). "GATA factor mutations in hematologic disease". Blood. 129 (15): 2103–2110. doi:10.1182/blood-2016-09-687889. PMC 5391620. PMID 28179280.
- Seewald L, Taub JW, Maloney KW, McCabe ER (September 2012). "Acute leukemias in children with Down syndrome". Molecular Genetics and Metabolism. 107 (1–2): 25–30. doi:10.1016/j.ymgme.2012.07.011. PMID 22867885.
- Reference list is found at image description page in Wikimedia Commons
- Clarke, RT; Van den Bruel, A; Bankhead, C; Mitchell, CD; Phillips, B; Thompson, MJ (October 2016). "Clinical presentation of childhood leukaemia: a systematic review and meta-analysis". Archives of Disease in Childhood. 101 (10): 894–901. doi:10.1136/archdischild-2016-311251. PMID 27647842.
- "Leukemia". Columbia Electronic Encyclopedia, 6th Edition. Retrieved 4 November 2011.
- American Cancer Society (2010). "How is Leukemia Diagnosed?". Detailed Guide: Leukemia – Adult Chronic. American Cancer Society. Archived from the original on 5 April 2010. Retrieved 4 May 2010.
- Ross JA, Kasum CM, Davies SM, Jacobs DR, Folsom AR, Potter JD (August 2002). "Diet and risk of leukemia in the Iowa Women's Health Study". Cancer Epidemiol. Biomarkers Prev. 11 (8): 777–81. PMID 12163333. Archived from the original on 10 September 2017.
- Radivoyevitch, T; Sachs, R K; Gale, R P; Molenaar, R J; Brenner, D J; Hill, B T; Kalaycio, M E; Carraway, H E; Mukherjee, S (2015). "Defining AML and MDS second cancer risk dynamics after diagnoses of first cancers treated or not with radiation". Leukemia. 30 (2): 285–294. doi:10.1038/leu.2015.258. PMID 26460209.
- Wiernik, Peter H. (2001). Adult leukemias. New York: B. C. Decker. pp. 3–15. ISBN 978-1-55009-111-3.
- Robinette, Martin S.; Cotter, Susan; Van de Water (2001). Quick Look Series in Veterinary Medicine: Hematology. Teton NewMedia. p. 105. ISBN 978-1-893441-36-1.
- Stass, Sanford A.; Schumacher, Harold R.; Rock, William R. (2000). Handbook of hematologic pathology. New York, N.Y: Marcel Dekker. pp. 193–194. ISBN 978-0-8247-0170-3.
- Leonard, Barry (1998). Leukemia: A Research Report. DIANE Publishing. p. 7. ISBN 978-0-7881-7189-5.
- Rudant J, Amigou A, Orsi L, Althaus T, Leverger G, Baruchel A, Bertrand Y, Nelken B, Plat G, Michel G, Sirvent N, Chastagner P, Ducassou S, Rialland X, Hémon D, Clavel J (2013). "Fertility treatments, congenital malformations, fetal loss, and childhood acute leukemia: the ESCALE study (SFCE)". Pediatr Blood Cancer. 60 (2): 301–8. doi:10.1002/pbc.24192. PMID 22610722.
- "Sr-90 is known to increase the risk of bone cancer and leukemia in animals, and is presumed to do so in people; from google (nuclear reactor emit tritium) result 1, 2, 3". Archived from the original on 20 July 2017.
- Pasmant, E; Ballerini, P; Lapillonne, H; Perot, C; Vidaud, D; Leverger, G; Landman-Parker, J (2009). "SPRED1 disorder and predisposition to leukemia in children". Blood. 114 (5): 1131. doi:10.1182/blood-2009-04-218503. PMID 19643996.
- Salesse, Stephanie; Verfaillie, Catherine M. (9 December 2002). "BCR/ABL: from molecular mechanisms of leukemia induction to treatment of chronic myelogenous leukemia". Oncogene. 21 (56): 8547–8559. doi:10.1038/sj.onc.1206082. ISSN 0950-9232. PMID 12476301.
- "NCI Dictionary of Cancer Terms". National Cancer Institute. 2 February 2011. Archived from the original on 16 February 2017. Retrieved 15 February 2017.
- "Do We Know What Causes Chronic Myeloid Leukemia?". www.cancer.org. Archived from the original on 16 February 2017. Retrieved 15 February 2017.
- "What is chronic myeloid leukaemia? (CML) - Understanding - Macmillan Cancer Support". www.macmillan.org.uk. Archived from the original on 16 February 2017. Retrieved 15 February 2017.
- Non-Ionizing Radiation, Part 1: Static and Extremely Low-Frequency (ELF) Electric and Magnetic Fields (IARC Monographs on the Evaluation of the Carcinogenic Risks). Geneva: World Health Organisation. 2002. pp. 332–333, 338. ISBN 978-92-832-1280-5. Archived from the original on 6 December 2008.
- "WHO | Electromagnetic fields and public health". Archived from the original on 16 February 2009. Retrieved 18 February 2009.
- Hoffbrand, A.V.; Moss, P.A.H.; Pettit, J.E. (2006). Essential haematology (5th ed.). Malden, Mass.: Blackwell Pub. ISBN 978-1-4051-3649-5.
- National Cancer Institute (1 January 1980). "Chronic Lymphocytic Leukemia (PDQ) Treatment: Stage Information". Archived from the original on 17 October 2007. Retrieved 4 September 2007.
- Eichhorst BF; Busch R; Hopfinger G; Pasold R; Hensel M; Steinbrecher C; Siehl S; Jäger U; Bergmann M; Stilgenbauer S; Schweighofer C; Wendtner CM; Döhner H; Brittinger G; Emmerich B; Hallek M; German CLL Study Group. (2006). "Fludarabine plus cyclophosphamide versus fludarabine alone in first-line therapy of younger patients with chronic lymphocytic leukemia". Blood. 107 (3): 885–91. doi:10.1182/blood-2005-06-2395. PMID 16219797.
- Gribben JG (January 2008). "Stem cell transplantation in chronic lymphocytic leukemia". Biol. Blood Marrow Transplant. 15 (1 Suppl): 53–8. doi:10.1016/j.bbmt.2008.10.022. PMC 2668540. PMID 19147079.
- American Cancer Society (22 March 2012). "Typical treatment of acute myeloid leukemia (except promyelocytic M3)". Detailed Guide: Leukemia – Acute Myeloid (AML). American Cancer Society. Archived from the original on 12 November 2012. Retrieved 31 October 2012.
- Fausel C (October 2007). "Targeted chronic myeloid leukemia therapy: seeking a cure" (PDF). J Manag Care Pharm. 13 (8 Suppl A): 8–12. PMID 17970609. Archived (PDF) from the original on 28 May 2008.
- Robak, T; Jamroziak, K; Gora-Tybor, J; Blonski, J. Z.; Kasznicki, M; Dwilewicz-Trojaczek, J; Wiater, E; Zdunczyk, A; Dybowicz, J; Dmoszynska, A; Wojtaszko, M; Zdziarska, B; Calbecka, M; Kostyra, A; Hellmann, A; Lewandowski, K; Stella-Holowiecka, B; Sulek, K; Gawronski, K; Skotnicki, A. B.; Nowak, W; Zawilska, K; Molendowicz-Portala, L; Kloczko, J; Sokolowski, J; Warzocha, K; Seferynska, I; Ceglarek, B; Konopka, L (2007). "Cladribine in a weekly versus daily schedule for untreated active hairy cell leukemia: Final report from the Polish Adult Leukemia Group (PALG) of a prospective, randomized, multicenter trial". Blood. 109 (9): 3672–5. doi:10.1182/blood-2006-08-042929. PMID 17209059.
- Saven, A; Burian, C; Adusumalli, J; Koziol, J. A. (1999). "Filgrastim for cladribine-induced neutropenic fever in patients with hairy cell leukemia". Blood. 93 (8): 2471–7. doi:10.1182/blood.V93.8.2471. PMID 10194424.
- Dearden CE, Matutes E, Cazin B (September 2001). "High remission rate in T-cell prolymphocytic leukemia with CAMPATH-1H". Blood. 98 (6): 1721–6. doi:10.1182/blood.V98.6.1721. PMID 11535503.
- "JMMLfoundation.org". JMMLfoundation.org. Archived from the original on 25 January 2009. Retrieved 29 August 2010.
- Stock, W (2010). "Adolescents and young adults with acute lymphoblastic leukemia". Hematology. American Society of Hematology. Education Program. 2010: 21–9. doi:10.1182/asheducation-2010.1.21. PMID 21239766.
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, Abraham J, Adair T, Aggarwal R, Ahn SY, Alvarado M, Anderson HR, Anderson LM, Andrews KG, Atkinson C, Baddour LM, Barker-Collo S, Bartels DH, Bell ML, Benjamin EJ, Bennett D, Bhalla K, Bikbov B, Bin Abdulhak A, Birbeck G, Blyth F, Bolliger I, Boufous S, Bucello C, Burch M, Burney P, Carapetis J, Chen H, Chou D, Chugh SS, Coffeng LE, Colan SD, Colquhoun S, Colson KE, Condon J, Connor MD, Cooper LT, Corriere M, Cortinovis M, de Vaccaro KC, Couser W, Cowie BC, Criqui MH, Cross M, Dabhadkar KC, Dahodwala N, De Leo D, Degenhardt L, Delossantos A, Denenberg J, Des Jarlais DC, Dharmaratne SD, Dorsey ER, Driscoll T, Duber H, Ebel B, Erwin PJ, Espindola P, Ezzati M, Feigin V, Flaxman AD, Forouzanfar MH, Fowkes FG, Franklin R, Fransen M, Freeman MK, Gabriel SE, Gakidou E, Gaspari F, Gillum RF, Gonzalez-Medina D, Halasa YA, Haring D, Harrison JE, Havmoeller R, Hay RJ, Hoen B, Hotez PJ, Hoy D, Jacobsen KH, James SL, Jasrasaria R, Jayaraman S, Johns N, Karthikeyan G, Kassebaum N, Keren A, Khoo JP, Knowlton LM, Kobusingye O, Koranteng A, Krishnamurthi R, Lipnick M, Lipshultz SE, Ohno SL, Mabweijano J, MacIntyre MF, Mallinger L, March L, Marks GB, Marks R, Matsumori A, Matzopoulos R, Mayosi BM, McAnulty JH, McDermott MM, McGrath J, Mensah GA, Merriman TR, Michaud C, Miller M, Miller TR, Mock C, Mocumbi AO, Mokdad AA, Moran A, Mulholland K, Nair MN, Naldi L, Narayan KM, Nasseri K, Norman P, O'Donnell M, Omer SB, Ortblad K, Osborne R, Ozgediz D, Pahari B, Pandian JD, Rivero AP, Padilla RP, Perez-Ruiz F, Perico N, Phillips D, Pierce K, Pope CA, Porrini E, Pourmalek F, Raju M, Ranganathan D, Rehm JT, Rein DB, Remuzzi G, Rivara FP, Roberts T, De León FR, Rosenfeld LC, Rushton L, Sacco RL, Salomon JA, Sampson U, Sanman E, Schwebel DC, Segui-Gomez M, Shepard DS, Singh D, Singleton J, Sliwa K, Smith E, Steer A, Taylor JA, Thomas B, Tleyjeh IM, Towbin JA, Truelsen T, Undurraga EA, Venketasubramanian N, Vijayakumar L, Vos T, Wagner GR, Wang M, Wang W, Watt K, Weinstock MA, Weintraub R, Wilkinson JD, Woolf AD, Wulf S, Yeh PH, Yip P, Zabetian A, Zheng ZJ, Lopez AD, Murray CJ, AlMazroa MA, Memish ZA (December 2012). "Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010". Lancet. 380 (9859): 2095–128. doi:10.1016/S0140-6736(12)61728-0. hdl:10536/DRO/DU:30050819. PMID 23245604.
- Mathers, Colin D, Cynthia Boschi-Pinto, Alan D Lopez and Christopher JL Murray (2001). "Cancer incidence, mortality and survival by site for 14 regions of the world" (PDF). Global Programme on Evidence for Health Policy Discussion Paper No. 13. World Health Organization.CS1 maint: multiple names: authors list (link)
- World Cancer Report 2014. World Health Organization. 2014. pp. Chapter 5.13. ISBN 978-9283204299.
- Amitay, EL; Keinan-Boker, L (1 June 2015). "Breastfeeding and Childhood Leukemia Incidence: A Meta-analysis and Systematic Review". JAMA Pediatrics. 169 (6): e151025. doi:10.1001/jamapediatrics.2015.1025. PMID 26030516.
- "Leukemia Facts & Statistics." Archived 16 April 2009 at the Wayback Machine The Leukemia & Lymphoma Society. Retrieved 2 July 2009.
- Horner MJ, Ries LAG, Krapcho M, Neyman N, et al. (eds). "SEER Cancer Statistics Review, 1975–2006". Surveillance Epidemiology and End Results (SEER). Bethesda, MD: National Cancer Institute. Archived from the original on 26 September 2009. Retrieved 3 November 2009.
Table 1.4: Age-Adjusted SEER Incidence and U.S. Death Rates and 5-Year Relative Survival Rates By Primary Cancer Site, Sex and Time Period
CS1 maint: multiple names: authors list (link) - James G. Gurney, Malcolm A. Smith, Julie A. Ross (1999) Cancer Incidence and Survival among Children and Adolescents, United States SEER program 1975–1995, chapter on Leukemia Archived 24 December 2010 at the Wayback Machine Cancer Statistics Branch, National Cancer Institute, available online from the SEER web site Archived 24 December 2010 at the Wayback Machine
- Childhood Blood Cancers | The Leukemia & Lymphoma Society Archived 5 September 2012 at the Wayback Machine
- Facts 2012 from The Leukemia & Lymphoma Society Archived 14 October 2012 at the Wayback Machine
- "Leukaemia (all subtypes combined) statistics". Cancer Research UK. Archived from the original on 7 October 2014. Retrieved 27 October 2014.
- Patlak, M (2002). "Targeting leukemia: From bench to bedside". FASEB Journal. 16 (3): 273. doi:10.1096/fj.02-0029bkt. PMID 11874976.
- "Leukemia: MedlinePlus Medical Encyclopedia". MedlinePlus. 8 May 2019. Retrieved 16 May 2019.
- Sontag, Susan (1978). Illness as Metaphor. New York: Farrar, Straus and Giroux. pp. 18. ISBN 978-0-374-17443-9.
- "A Snapshot of Leukemia". NCI. Archived from the original on 4 July 2014. Retrieved 18 June 2014.
- "Search of: leukemia — List Results — ClinicalTrials.gov". Archived from the original on 15 September 2010.
- "Understanding Clinical Trials for Blood Cancers" (PDF). Leukemia and Lymphoma Society. Archived from the original (PDF) on 5 January 2011. Retrieved 19 May 2010.
- Jaslow, Ryan. "New Leukemia Therapy Destroys Cancer by Turning Blood Cells into "Assassins"". CBSnews.com HealthPop section. Archived from the original on 31 March 2014. Retrieved 11 August 2011.
- Coghlan, Andy (26 March 2013) Gene therapy cures leukaemia in eight days Archived 15 May 2015 at the Wayback Machine The New Scientist, Retrieved 15 April 2013
- Zhao, Juanjuan; Song, Yongping; Liu, Delong (14 February 2019). "Clinical trials of dual-target CAR T cells, donor-derived CAR T cells, and universal CAR T cells for acute lymphoid leukemia". Journal of Hematology & Oncology. 12 (1): 17. doi:10.1186/s13045-019-0705-x. ISSN 1756-8722. PMC 6376657. PMID 30764841.
- Zheng, Ping-Pin; Kros, Johan M.; Li, Jin (2018). "Approved CAR T cell therapies: ice bucket challenges on glaring safety risks and long-term impacts". Drug Discovery Today. 23 (6): 1175–1182. doi:10.1016/j.drudis.2018.02.012. hdl:1765/105338. PMID 29501911.
- "How we're beating leukaemia". Leukaemia & Lymphoma Research. Archived from the original on 27 September 2013. Retrieved 24 September 2013.
- Shapira T, Pereg D, Lishner M (September 2008). "How I treat acute and chronic leukemia in pregnancy". Blood Rev. 22 (5): 247–59. doi:10.1016/j.blre.2008.03.006. PMID 18472198.
- Koren G, Lishner M (2010). "Pregnancy and commonly used drugs in hematology practice". Hematology Am Soc Hematol Educ Program. 2010: 160–5. doi:10.1182/asheducation-2010.1.160. PMID 21239787.
{kind=link}
External links
| Classification | |
|---|---|
| External resources |
|
| Wikimedia Commons has media related to Leukemias. |
- Leukemia at Curlie
- Leukaemia information from Cancer Research UK
| Authority control |
|
|---|