Uterine incarceration
Uterine incarceration is an obstetrical complication whereby a growing retroverted uterus becomes wedged into the pelvis after the first trimester of pregnancy.[1]
| Uterine incarceration during pregnancy | |
|---|---|
 | |
| Specialty | Obstetrics |
Causes
A number of situations may interfere with the natural process that would antevert a retroverted uterus during pregnancy. Such situations include pelvic adhesions, endometriosis, uterine malformations, leiomyomata, and pelvic tumors.[2]
Development
When the uterus is tilted backwards, it is considered to be retroverted; this situation is common and regarded a normal variation. It has been estimated that about 15% of pregnancies begin in a retroverted uterus.[3] Normally, during the first trimester, the growing uterus changes spontaneously to an anteverted position, thus allowing expansion of the enlarging uterus into the abdomen. The cervix is then inferior to the body of the uterus. Thus, the presence of an early pregnancy in a retroverted uterus is not considered a problem.[1]
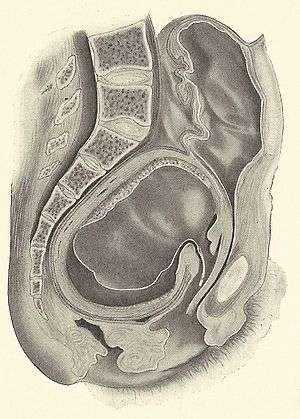
On rare occasions the uterus fails to become anteverted, and the pregnancy continues to expand the retroverted uterus within the confines of the pelvis. By about 14 weeks the size of the uterus fills out most of the pelvis, pushing up the cervix. At this point the uterus may get trapped below the sacral promontory and symphysis. With further growth the pregnant woman may experience lower abdominal and pelvic pain, back pain, and difficulty, even inability to void, as the bladder is pushed upward and its outflow becomes obstructed. Constipation may be encountered. The frequency of this complication has been estimated to be about 1 in 3,000 pregnancies.[2]
Diagnosis
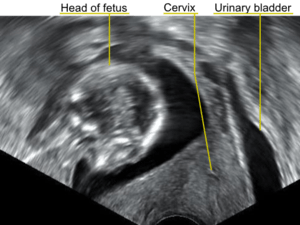
In a pregnant woman who is entering her second trimester, the combination of urinary difficulties and pelvic pain may alert the physician to consider uterine incarceration as a possibility. On physical examination, the cervix is pushed up and anterior, and the pelvis entirely filled by the soft mass of the body of the pregnant uterus. Sonography may indicate the retroverted position of the uterus, check on the viability of the fetus, and demonstrate the location of the bladder being pushed cranially and unable to be emptied.[4] Also magnetic resonance imaging has been found to be helpful in the diagnosis of the condition.[4][5]
Sequelae
Spontaneous resolution of the condition can occur during the second trimester.[6] An unresolved incarcerated uterus can lead to further pain, vaginal bleeding, loss of pregnancy or premature delivery. Also, the uterus may develop a uterine sacculation, that is a part of its back wall softens like an aneurysm and allows expansion of the fetus into the abdomen with a risk of uterine rupture.[3] Further, urinary complications may develop such as cystitis, and bladder distention could eventually lead to rupture of the bladder.[7]
Management
A pregnant woman with an incarcerated uterus may present in the emergency room because of pain, bleeding, inability to void and constipation. Upon diagnosis steps can be taken to manually position the uterus into an anteverted position. The bladder is decompressed by a Foley catheter and the obstetrician may attempt to manipulate the uterus if necessary using general or spinal anesthesia.[3] Rarely will a woman with an incarcerated uterus reach term, - if so, a cesarean delivery is called for.[8]
References
- Lettieri L, Rodis JF, McLean DA, Campbell WA, Vintzileos AM (September 1994). "Incarceration of the gravid uterus". Obstet. Gynecol. Surv. 49 (9): 642–6. PMID 7991232.
- van der Tuuk K, Krenning RA, Krenning G, Monincx WM (2009). "Recurrent incarceration of the retroverted gravid uterus at term - two times transvaginal caesarean section: a case report". Journal of Medical Case Reports. 3 (1): 103. doi:10.1186/1752-1947-3-103. PMC 2783044. PMID 19946581.
- Amy N. Sweigart; Michael J. Matteucci (2008). "Fever, Sacral Pain, and Pregnancy: An Incarcerated Uterus". West J Emerg Med. 9 (4): 232–4. PMC 2672273. PMID 19561753.
- Fernandes DD, Sadow CA, Economy KE, Benson CB (April 2012). "Sonographic and magnetic resonance imaging findings in uterine incarceration". J Ultrasound Med. 31 (4): 645–50. PMID 22441922.
- Hachisuga N, Hidaka N, Fujita Y, Fukushima K, Wake N (2012). "Significance of pelvic magnetic resonance imaging in preoperative diagnosis of incarcerated retroverted gravid uterus with a large anterior leiomyoma: a case report". J Reprod Med. 57 (1–2): 77–80. PMID 22324275.
- Rose CH, Brost BC, Watson WJ, Davies NP, Knudsen JM (January 2008). "Expectant management of uterine incarceration from an anterior uterine myoma: a case report". J Reprod Med. 53 (1): 65–6. PMID 18251368.
- J. Whitridge Williams. Obstetrics. D. Appleton and Co, 1906. p. 474.
- Al Wadi K, Helewa M, Sabeski L (July 2011). "Asymptomatic uterine incarceration at term: a rare complication of pregnancy". J Obstet Gynaecol Can. 33 (7): 729–32. PMID 21749750.