Hyperplasia
Hyperplasia (from ancient Greek ὑπέρ huper, "over" + πλάσις plasis, "formation"), or hypergenesis, is an increase in the amount of organic tissue that results from cell proliferation.[4] It may lead to the gross enlargement of an organ, and the term is sometimes confused with benign neoplasia or benign tumor.[5]
| Hyperplasia | |
|---|---|
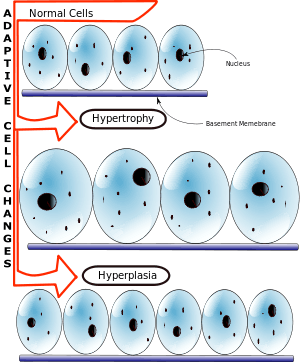 | |
| Whereas hypertrophy stems from an increase in cell size, hyperplasia results from an increase in cell number. | |
| Specialty | Pathology |
| Types | Benign prostatic hyperplasia, Hyperplasia of the breast(many more)[1][2] |
| Diagnostic method | Biopsy[3] |
| Treatment | Depends which type (see types) |
Hyperplasia is a common preneoplastic response to stimulus.[6] Microscopically, cells resemble normal cells but are increased in numbers. Sometimes cells may also be increased in size (hypertrophy).[7] Hyperplasia is different from hypertrophy in that the adaptive cell change in hypertrophy is an increase in the size of cells, whereas hyperplasia involves an increase in the number of cells.[8]
Signs and symptoms
Hyperplasia is considered to be a physiological (normal) response to a specific stimulus, and the cells of a hyperplastic growth remain subject to normal regulatory control mechanisms.[5] However, hyperplasia can also occur as a pathological response, if an excess of hormone or growth factor is responsible for the stimuli. Similarly to physiological hyperplasia, cells that undergo pathologic hyperplasia are controlled by growth hormones, and cease to proliferate if such stimuli are removed.[9] This differs from neoplasia (the process underlying cancer and benign tumors), in which genetically abnormal cells manage to proliferate in a non-physiological manner which is unresponsive to normal stimuli.[10] That being said, the effects caused by pathologic hyperplasia can provide a suitable foundation from which neoplastic cells may develop.[9]
| -plasia and -trophy |
|---|
|
|
Causes
Hyperplasia may be due to any number of causes, including proliferation of basal layer of epidermis to compensate skin loss, chronic inflammatory response, hormonal dysfunctions, or compensation for damage or disease elsewhere.[11] Hyperplasia may be harmless and occur on a particular tissue. An example of a normal hyperplastic response would be the growth and multiplication of milk-secreting glandular cells in the breast as a response to pregnancy, thus preparing for future breast feeding.[12]
Perhaps the most interesting and potent effect IGF has on the human body is its ability to cause hyperplasia, which is an actual splitting of cells.[13] By contrast, hypertrophy is what occurs, for example, to skeletal muscle cells during weight training and steroid use and is simply an increase in the size of the cells.[14] With IGF use, one is able to cause hyperplasia which actually increases the number of muscle cells present in the tissue.[15] Weight training with or without anabolic steroid use enables these new cells to mature in size and strength. It is theorized that hyperplasia may also be induced through specific power output training for athletic performance, thus increasing the number of muscle fibers instead of increasing the size of a single fiber.[16]
Diagnosis
In the case of endometrial hyperplasia usually a Pap smear is done, also a biopsy during the pelvic examination, may be done of the individuals endometrial tissue. You may want to consult your doctor for further examination.[3] In regards to Cushing's disease, the diagnosis of salivary cortisol in an elevated level around "late-night" is a way to detect it in many patients.[17]
Types

Some of the more commonly known clinical forms of hyperplasia, or conditions leading to hyperplasia, are:
- Benign prostatic hyperplasia, also known as prostate enlargement.[1]
- Cushing's disease – Physiopathology of hyperplasia of adrenal cortex due to increased circulating level of ACTH (adrenocorticotropic hormone).[18]
- Congenital adrenal hyperplasia – Inherited disorder of gland (adrenal).[19]
- Endometrial hyperplasia – Hyperproliferation of the endometrium, usually in response to unopposed estrogen stimulation in the setting of polycystic ovary syndrome or exogenous administration of hormones. Atypical endometrial hyperplasia may represent an early neoplastic process which can lead to endometrial adenocarcinoma.[20] The development of endometrial adenocarcinoma from endometrial hyperplasia is a typical example of how the effects of pathologic hyperplasia can lead to neoplasia, and females who exhibit hyperplasia of the endometrium are indeed more likely to develop cancer of these cells.[9]
- Hemihyperplasia when only half (or one side) of the body is affected, sometimes generating limbs of different lengths.[21]
- Hyperplasia of the breast – "Hyperplastic" lesions of the breast include usual ductal hyperplasia, a focal expansion of the number of cells in a terminal breast duct, and atypical ductal hyperplasia, in which a more abnormal pattern of growth is seen, and which is associated with an increased risk of developing breast cancer.[2]
- Intimal hyperplasia – The thickening of the tunica intima of a blood vessel as a complication of a reconstruction procedure or endarterectomy. Intimal hyperplasia is the universal response of a vessel to injury and is an important reason of late bypass graft failure, particularly in vein and synthetic vascular grafts.[22]
- Focal epithelial hyperplasia (also known as Heck's disease) – This is a wart-like growth in the mucous tissues of the mouth or, rarely, throat that is caused by certain sub-types of the human papillomavirus (HPV). Heck's disease has not been known to cause cancer.[23]
- Sebaceous hyperplasia – In this condition, small yellowish growths develop on the skin, usually on the face. This condition is neither contagious nor dangerous.[24]
- Compensatory liver hyperplasia – The liver undergoes cellular division after acute injury, resulting in new cells that restore liver function back to baseline. Approximately 75% of the liver can be acutely damaged or resected with seemingly full regeneration through hepatocyte division, i.e., hyperplasia. This is what makes living-donor liver transplants possible.[25]
Treatment
The treatment of hyperplasia would consist upon which; in the case of benign prostate hyperplasia the combination of alpha-1-receptor blockers and 5-alpha-reductase inhibitors are effective.[26]
See also
- List of biological development disorders
References
- "Prostate Enlargement: Benign Prostatic Hyperplasia". www.niddk.nih.gov. Retrieved 2015-05-30.
- Koerner, Frederick C. (2009). Diagnostic Problems in Breast Pathology. Elsevier Health Sciences. ISBN 978-1416026129.
- Dunphy, Lynne M.; Winland-Brown, Jill E. (2011-04-06). Primary Care: The Art and Science of Advanced Practice Nursing. F.A. Davis. ISBN 9780803626478.
- "Hyperplasia: MedlinePlus Medical Encyclopedia". www.nlm.nih.gov. Retrieved 2015-05-30.
- Sembulingam, K.; Sembulingam, Prema (2012-09-01). Essentials of Medical Physiology. JP Medical Ltd. ISBN 9789350259368.
- Zachary, James F.; McGavin, M. Donald (2013-12-11). Pathologic Basis of Veterinary Disease. Elsevier Health Sciences. ISBN 9780323291729.
- Braun, Carie Ann; Anderson, Cindy Miller (2007). Pathophysiology: Functional Alterations in Human Health. Lippincott Williams & Wilkins. ISBN 9780781762502.
- Rubin, Emanuel; Reisner, Howard M. (2009). Essentials of Rubin's Pathology. Lippincott Williams & Wilkins. ISBN 9780781773249.
- Kumar, V., Abbas, A., Aster, J. (2013). Robbins Basic Pathology. Philadelphia, USA: Elsevier. p. 4. ISBN 9780808924326.CS1 maint: multiple names: authors list (link)
- Hong, Waun Ki; Hait, William N. (2010). Holland Frei Cancer Medicine Eight. PMPH-USA. ISBN 9781607950141.
- Porth, Carol (2011). Essentials of Pathophysiology: Concepts of Altered Health States. Lippincott Williams & Wilkins. ISBN 9781582557243.
- Dirbas, Frederick; Scott-Conner, Carol (2011-01-15). Breast Surgical Techniques and Interdisciplinary Management. Springer Science & Business Media. ISBN 9781441960764.
- Gardiner, Phillip. Advanced Neuromuscular Exercise Physiology. Human Kinetics. ISBN 9781450412278.
- Metzl, Jordan D.; Shookhoff, Carol (2009-10-31). The Young Athlete: A Sports Doctor's Complete Guide for Parents. Little, Brown. ISBN 9780316086738.
- Publishing, Britannica Educational (2011-11-01). The Endocrine System. Britannica Educational Publishing. ISBN 9781615307319.
- Kisner, Carolyn; Colby, Lynn Allen (2012-10-08). Therapeutic Exercise: Foundations and Techniques. F.A. Davis. ISBN 9780803638976.
- Cushing's Syndrome: New Insights for the Healthcare Professional: 2013 Edition: ScholarlyBrief. ScholarlyEditions. 2013-07-22. ISBN 9781481651837.
- "Cushing disease: MedlinePlus Medical Encyclopedia". www.nlm.nih.gov. Retrieved 2015-05-30.
- "Congenital adrenal hyperplasia: MedlinePlus Medical Encyclopedia". www.nlm.nih.gov. Retrieved 2015-05-30.
- "Endometrial Hyperplasia - ACOG". www.acog.org. Retrieved 2015-05-30.
- "Hemihyperplasia - Glossary Entry". Genetics Home Reference. Retrieved 2015-05-30.
- Subbotin, Vladimir M (2007-10-31). "Analysis of arterial intimal hyperplasia: review and hypothesis". Theoretical Biology & Medical Modelling. 4: 41. doi:10.1186/1742-4682-4-41. ISSN 1742-4682. PMC 2169223. PMID 17974015.
- Purkait, Swapan Kumar (2011). Essentials of Oral Pathology. JP Medical Ltd. ISBN 9789350252147.
- Evans, Colby Craig; High, Whitney A. (2011-10-01). Skin Diseases in the Elderly: A Color Handbook. CRC Press. ISBN 9781840766158.
- Kumar, Vinay; Abbas, Abul K.; Aster, Jon C. (2014-09-05). Robbins & Cotran Pathologic Basis of Disease. Elsevier Health Sciences. ISBN 9780323296359.
- "Benign Prostatic Hypertrophy Treatment & Management: Approach Considerations, Combination Therapy, Minimally Invasive Treatment". Medscape. eMedicine. Retrieved 3 September 2016.
Further reading
- Bachmann, Alexander; Rosette, Jean de la (2011-11-24). Benign Prostatic Hyperplasia and Lower Urinary Tract Symptoms in Men. OUP Oxford. ISBN 9780199572779.
External links
| Classification |
|
|---|---|
| External resources |