Healthcare in Germany
Germany has a universal[1] multi-payer health care system paid for by a combination of statutory health insurance (Gesetzliche Krankenversicherung) and "Private Krankenversicherung" (private health insurance).[2][3][4][5][6]
_4.jpg)
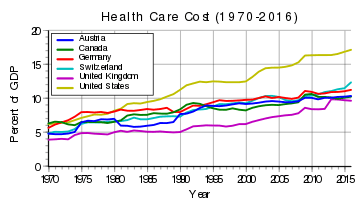
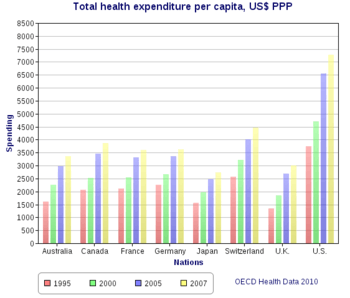
The turnover of the health sector was about US$368.78 billion (€287.3 billion) in 2010, equivalent to 11.6 percent of gross domestic product (GDP) and about US$4,505 (€3,510) per capita.[7] According to the World Health Organization, Germany's health care system was 77% government-funded and 23% privately funded as of 2004.[8] In 2004 Germany ranked thirtieth in the world in life expectancy (78 years for men). It had a very low infant mortality rate (4.7 per 1,000 live births), and it was tied for eighth place in the number of practicing physicians, at 3.3 per 1,000 persons. In 2001 total spending on health amounted to 10.8 percent of gross domestic product.[9]
According to the Euro health consumer index, which placed it in seventh position in its 2015 survey, Germany has long had the most restriction-free and consumer-oriented healthcare system in Europe. Patients are allowed to seek almost any type of care they wish whenever they want it.[10] The governmental health system in Germany is currently keeping a record reserve of more than €18,000,000,000 which makes it one of the healthiest healthcare systems in the world.[11]
History
Germany has the world's oldest national social health insurance system,[1] with origins dating back to Otto von Bismarck's social legislation, which included the Health Insurance Bill of 1883, Accident Insurance Bill of 1884, and Old Age and Disability Insurance Bill of 1889. Bismarck stressed the importance of three key principles; solidarity, the government is responsible for ensuring access by those who need it, subsidiarity, policies are implemented with smallest no political and administrative influence, and corporatism, the government representative bodies in health care professions set out procedures they deem feasible.[12] Mandatory health insurance originally applied only to low-income workers and certain government employees, but has gradually expanded to cover the great majority of the population.[13] The system is decentralized with private practice physicians providing ambulatory care, and independent, mostly non-profit hospitals providing the majority of inpatient care. Approximately 92% of the population are covered by a 'Statutory Health Insurance' plan, which provides a standardized level of coverage through any one of approximately 1,100 public or private sickness funds. Standard insurance is funded by a combination of employee contributions, employer contributions and government subsidies on a scale determined by income level. Higher-income workers sometimes choose to pay a tax and opt-out of the standard plan, in favor of 'private' insurance. The latter's premiums are not linked to income level but instead to health status.[14] Historically, the level of provider reimbursement for specific services is determined through negotiations between regional physicians' associations and sickness funds.
1970–Present
Since 1976 the government has convened an annual commission, composed of representatives of business, labor, physicians, hospitals, and insurance and pharmaceutical industries.[15] The commission takes into account government policies and makes recommendations to regional associations with respect to overall expenditure targets. In 1986 expenditure caps were implemented and were tied to the age of the local population as well as the overall wage increases. Although reimbursement of providers is on a fee-for-service basis the amount to be reimbursed for each service is determined retrospectively to ensure that spending targets are not exceeded. Capitated care, such as that provided by U.S. health maintenance organizations, has been considered as a cost-containment mechanism but would require consent of regional medical associations, and has not materialized.[16]
Copayments were introduced in the 1980s in an attempt to prevent overutilization and control costs. The average length of hospital stay in Germany has decreased in recent years from 14 days to 9 days, still considerably longer than average stays in the U.S. (5 to 6 days).[17][18] The difference is partly driven by the fact that hospital reimbursement is chiefly a function of the number of hospital days as opposed to procedures or the patient's diagnosis. Drug costs have increased substantially, rising nearly 60% from 1991 through 2005. Despite attempts to contain costs, overall health care expenditures rose to 10.7% of GDP in 2005, comparable to other western European nations, but substantially less than that spent in the U.S. (nearly 16% of GDP).[19]
Regulation
The healthcare system is regulated by the Federal Joint Committee (Gemeinsamer Bundesausschuss), a public health organization authorized to make binding regulations growing out of health reform bills passed by lawmakers, along with routine decisions regarding healthcare in Germany.[20] The Federal Joint Committee consists of 13 members, who are entitled to vote on these binding regulations. The members composed of legal representatives of the public health insurances, the hospitals, the doctors and dentists and three impartial members. Also, there are five representatives of the patients with an advisory role who are not allowed to vote.
The German law about the public health insurance (Fünftes Sozialgesetzbuch) sets the framework agreement for the committee. One of the most important tasks is to decide which treatments and performances the insurances have to pay for by law. The principle about these decisions is that every treatment and performance has to be required, economic, sufficient and appropriate. [21]
Health insurance
Health insurance is compulsory for the whole population in Germany; in 2009, coverage was expanded from nearly all the population to everyone.[22]
Salaried workers and employees below the relatively high income threshold of 60,750 Euros per year (2019)[23] are automatically enrolled into one of currently around 130 public non-profit "sickness funds" at common rates for all members, and is paid for with joint employer-employee contributions. The employer pays half of the contribution, and the employee pays the other half.[23] Self-employed workers must pay the entire contribution themselves. Provider payment is negotiated in complex corporatist social bargaining among specified self-governed bodies (e.g. physicians' associations) at the level of federal states (Länder). The sickness funds are mandated to provide a unique and broad benefit package and cannot refuse membership or otherwise discriminate on an actuarial basis. Social welfare beneficiaries are also enrolled in statutory health insurance, and municipalities pay contributions on behalf of them.
Besides the "Statutory Health Insurance" (Gesetzliche Krankenversicherung) covering the vast majority of residents, those with a yearly income above 60,750 Euros (2019), students and civil servants for complementary coverage can opt for private health insurance (about 11% of the population have private health insurance). Most civil servants benefit from a tax-funded government employee benefit scheme covering a percentage of the costs, and cover the rest of the costs with a private insurance contract. Recently, private insurers provide various types of supplementary coverage as an add upon of the SHI benefit package (e.g. for glasses, coverage abroad and additional dental care or more sophisticated dentures). Health insurance in Germany is split in several parts. The largest part of 89% of the population is covered by a comprehensive health insurance plan provided by statutory public health insurance funds regulated under specific the legislation set with the Sozialgesetzbuch V (SGB V), which defines the general criteria of coverage, which are translated into benefit packages by the Federal Joint Committee. The remaining 11% opt for private health insurance, including government employees.[24]
Public health insurance contributions are based on the worker's salary. Private insurers charge risk-related contributions.[23] This may result in substantial savings for younger individuals in good health. With age, private contributions tend to rise and a number of insurees formerly cancelled their private insurance plan in order to return to statutory health insurance; this option is now only possible for beneficiaries under 55 years.[14][25]
Reimbursement for outpatient care was on a fee-for-service basis but has changed into basic capitation according to the number of patients seen during one quarter, with a capped overall spending for outpatient treatments and region. Moreover, regional panel physician associations regulate number of physicians allowed to accept Statutory Health Insurance in a given area. Co-payments, which exist for medicines and other items are relatively low compared to other countries.
Insurance systems
Germany has a universal system with two main types of health insurance. Germans are offered three mandatory health benefits, which are co-financed by employer and employee: health insurance, accident insurance, and long-term care insurance.
Accident insurance for working accidents (Arbeitsunfallversicherung) is covered by the employer and basically covers all risks for commuting to work and at the workplace.
Long-term care (Pflegeversicherung) is covered half and half by employer and employee and covers cases in which a person is not able to manage his or her daily routine (provision of food, cleaning of apartment, personal hygiene, etc.). It is about 2% of a yearly salaried income or pension, with employers matching the contribution of the employee.
There are two separate types of health insurance: public health insurance (Gesetzliche Krankenversicherung) and private insurance (Private Krankenversicherung). Both systems struggle with the increasing cost of medical treatment and the changing demography. About 87.5% of the persons with health insurance are members of the public system, while 12.5% are covered by private insurance (as of 2006).[26]
In 2013 a state funded private care insurance was introduced ("Private Pflegeversicherung").[27] Insurance contracts that fit certain criteria are subsidised with 60 Euro per year. It is expected that the number of contracts will grow from 400,000 by end of 2013 to over a million within the next few years.[28] These contracts have been criticized by consumer rights foundations.[29]
Insuring organizations
The German legislature has reduced the number of public health insurance organisations from 1209 in 1991 down to 123 in 2015.[30]
The public health insurance organisations (Krankenkassen) are the Ersatzkassen (EK), Allgemeine Ortskrankenkassen (AOK), Betriebskrankenkassen (BKK), Innungskrankenkassen (IKK), Knappschaft (KBS), and Landwirtschaftliche Krankenkasse (LKK).[31]
As long as a person has the right to choose his or her health insurance, he or she can join any insurance that is willing to include the individual.
| public health insurance organisations in January 2019[32] | Numbers | number of members including retired persons | open on federal level | open on state level | not open |
|---|---|---|---|---|---|
| all public insurance organisations | 109 | 72.8 M | 43 | 46 | 29 |
| Betriebskrankenkassen | 84 | 10.9 M | 33 | 32 | 28 |
| Allgemeine Ortskrankenkassen | 11 | 26.5 M | 0 | 11 | 0 |
| Landwirtschaftliche Krankenkassen | 1 | 0.6 M | 0 | 0 | 1 |
| Ersatzkassen | 6 | 28.0 M | 6 | 0 | 0 |
| Innungskrankenkassen | 6 | 5.2 M | 3 | 3 | 0 |
| Knappschaft | 1 | 1.6 M | 1 | 0 | 0 |
Public insurance

Regular salaried employees must have public health insurance, unless their income exceeds 60,750€ per year (2019). If their income exceeds that amount, they can have private health insurance instead. Freelancers can have public or private insurance, regardless of their income.[23]
In the Public system the premium
- is set by the Federal Ministry of Health based on a fixed set of covered services as described in the German Social Law (Sozialgesetzbuch – SGB), which limits those services to "economically viable, sufficient, necessary and meaningful services"
- is not dependent on an individual's health condition, but a percentage (currently 15.5%, 7.3% of which is covered by the employer) of salaried income under €54,450 per year (in 2019).[23]
- includes family members of any family members, or "registered member" ( Familienversicherung – i.e., husband/wife and children are free)
- is a "pay as you go" system – there is no saving for an individual's higher health costs with rising age or existing conditions.
Private insurance
In the Private system the premium
- is based on an individual agreement between the insurance company and the insured person defining the set of covered services and the percentage of coverage
- depends on the amount of services chosen and the person's risk and age of entry into the private system
- is used to build up savings for the rising health costs at higher age (required by law)
For persons who have opted out of the public health insurance system to get private health insurance, it can prove difficult to subsequently go back to the public system, since this is only possible under certain circumstances, for example if they are not yet 55 years of age and their income drops below the level required for private selection. Since private health insurance is usually more expensive than public health insurance, the higher premiums must then be paid out of a lower income. During the last twenty years private health insurance became more and more expensive and less efficient compared with the public insurance.
In Germany, all privately financed products and services for health are assigned as part of the 'second health market'.[33] Unlike the 'first health market' they are usually not paid by a public or private health insurance. Patients with public health insurance paid privately about 1.5 Billion Euro in this market segment in 2011, while already 82% of physicians offered their patients in their practices individual services being not covered by the patient's insurances; the benefits of these services are controversial discussed.[34] Private investments in fitness, for wellness, assisted living, and health tourism are not included in this amount. The 'second health market' in Germany is compared to the United States still relatively small, but is growing continuously.
Self-payment (International patients without any national insurance coverage)
Besides the primary governmental health insurance and the secondary private health insurance mentioned above, all governmental and private clinics generally work in an inpatient setting with a prepayment-system, requiring a cost-estimate that needs to be covered before the perspective therapy can be planned. Several university hospitals in Germany have therefore country-specific quotes for pre-payments that can differ from 100% to the estimated costs and the likelihood of unexpected additional costs, i.e. due to risks for medical complications.[35][36]
Economics
Health economics in Germany can be considered as a collective term for all activities that have anything to do with health in this country.[37] This interpretation done by Andreas Goldschmidt in 2002 seems, however, very generous due to several overlaps with other economic sectors.[38] A simple outline of the health sector in three areas provides an "onion model of health care economics" by Elke Dahlbeck and Josef Hilbert[39] from "Institut Arbeit und Technik (IAT)" at the University of applied sciences Gelsenkirchen:[40] Core area is the ambulatory and inpatient acute care and geriatric care, and health administration. Around it is located wholesale and supplier sector with pharmaceutical industry, medical technology, healthcare, and wholesale trade of medical products. Health-related margins are the fitness and spa facilities, assisted living, and health tourism.
According to this basic idea, an almost totally regulated health care market like in the UK were not very productive, but also a largely deregulated market in the United States would not be optimal. Both systems would suffer concerning sustainable and comprehensive patient care. Only a hybrid of social well-balanced and competitive market conditions created a relevant optimum.[41] Nevertheless, forces of the healthcare market in Germany are often regulated by a variety of amendments and health care reforms at the legislative level, especially by the "Social Security Code" (Sozialgesetzbuch- SGB) in the past 30 years.
Health care in Germany, including its industry and all services, is one of the largest sectors of the German economy. Direct inpatient and outpatient care equivalent to just about a quarter of the entire 'market' - depending on the perspective.[7] A total of 4.4 million people working in this, that means about one in ten employees in 2007 and 2008.[42] The total expenditure in health economics was about 287.3 billion Euro in Germany in 2010, equivalent to 11.6 percent of gross domestic product (GDP) this year and about 3.510 Euro per capita.[43]
Drugs costs
The pharmaceutical industry plays a major role in Germany within and beyond direct health care. Expenditure on pharmaceutical drugs is almost half of those for the entire hospital sector. Pharmaceutical drug expenditure grew by an annual average of 4.1% between 2004 and 2010. Such developments caused numerous health care reforms since the 1980s. An actual example of 2010 and 2011: First time since 2004 the drug expenditure fell from 30.2 billion Euro in 2010 to 29.1 billion Euro in 2011, i. e. minus 1.1 billion Euro or minus 3.6%. That was caused by restructuring the Social Security Code: manufacturer discount 16% instead of 6%, price moratorium, increasing discount contracts, increasing discount by wholesale trade and pharmacies.[44]
As of 2010, Germany has used reference pricing and incorporates cost sharing to charge patients more when a drug is newer and more effective than generic drugs.[45] However, as of 2013 total out-of-costs for medications are capped at 2% of income, and 1% of income for people with chronic diseases.[46]
Statistics
.jpg)
In a sample of 13 developed countries Germany was seventh in its population weighted usage of medication in 14 classes in 2009 and tenth in 2013. The drugs studied were selected on the basis that the conditions treated had high incidence, prevalence and/or mortality, caused significant long-term morbidity and incurred high levels of expenditure and significant developments in prevention or treatment had been made in the last 10 years. The study noted considerable difficulties in cross border comparison of medication use.[47] It has the highest number of dentists in Europe - 64,287 in 2015.[48]
Major diagnosis
In 2002 the top diagnosis for male patients released from the hospital was heart disease, followed by alcohol-related disorders and hernias. For women, the top diagnoses related to pregnancies, breast cancer, and heart disease.
Hospitals

The average length of hospital stay in Germany has decreased in recent years from 14 days to 9 days, still considerably longer than average stays in the United States (5 to 6 days).[49][50] Part of the difference is that the chief consideration for hospital reimbursement is the number of hospital days as opposed to procedures or diagnosis. Drug costs have increased substantially, rising nearly 60% from 1991 through 2005. Despite attempts to contain costs, overall health care expenditures rose to 10.7% of GDP in 2005, comparable to other western European nations, but substantially less than that spent in the U.S. (nearly 16% of GDP).[51]
In 2017 the BBC reported that compared with the United Kingdom the Caesarean rate, the use of MRI for diagnosis and the length of hospital stay are all higher in Germany.[52]
Waiting times
According to several sources from the past decade, waiting times in Germany remain low for appointments and surgery, although a minority of elective surgery patients face longer waits. In 1992, a study by Fleming et al. (cited in Siciliani & Hurst, 2003, p. 8),[53] 19.4% of German respondents said they'd waited more than 12 weeks for their surgery.
In the Commonwealth Fund 2010 Health Policy Survey in 11 Countries, Germany reported some of the lowest waiting times. Germans had the highest percentage of patients reporting their last specialist appointment took less than 4 weeks (83%, v. 80% for the U. S.), and the second-lowest reporting it took 2 months or more (7%, vs. 5% for Switzerland and 9% for the U. S.). 70% of Germans reported that they waited less than 1 month for elective surgery, the highest percentage, and the lowest percentage (0%) reporting it took 4 months or more.[54]
Both Social Health Insurance (SHI) and privately insured patient experienced low waits, but privately insured patients' waits were even lower. According to the Kassenärztliche Bundesvereinigung (KBV), the body representing contract physicians and contract psychotherapists at federal level, 56% of Social Health Insurance patients waited 1 week or less, while only 13% waited longer than 3 weeks for a doctor's appointment. 67% of privately insured patients waited 1 week or less, while 7% waited longer than 3 weeks.[55] Waits can also vary somewhat by region. Waits were longer in eastern Germany according to the KBV (KBV, 2010), as cited in "Health at a Glance 2011: OECD Indicators".[56]
Germany has a large hospital sector capacity measured in beds. High capacity on top of significant day surgery outside of hospitals (especially for ophthalmology and othopaedic surgery) with doctors paid fee-for-service for activity performed are likely factors preventing long waits, despite hospital budget limitations.[53] Activity-based payment for hospitals also is linked to low waiting times (Siciliani & Hurst, 2003, 33-34, 70).[53] Germany introduced Diagnosis-Related Group activity-based payment for hospitals (with a soft cap budget limit).[57]
See also
References
- Bump, Jesse B. (October 19, 2010). "The long road to universal health coverage. A century of lessons for development strategy" (PDF). Seattle: PATH. Retrieved March 10, 2013.
Carrin and James have identified 1988—105 years after Bismarck’s first sickness fund laws—as the date Germany achieved universal health coverage through this series of extensions to growing benefit packages and expansions of the enrolled population. Bärnighausen and Sauerborn have quantified this long-term progressive increase in the proportion of the German population covered mainly by public and to a smaller extent by private insurance. Their graph is reproduced below as Figure 1: German Population Enrolled in Health Insurance (%) 1885–1995.
Carrin, Guy; James, Chris (January 2005). "Social health insurance: Key factors affecting the transition towards universal coverage" (PDF). International Social Security Review. 58 (1): 45–64. doi:10.1111/j.1468-246X.2005.00209.x. Retrieved March 10, 2013.Initially the health insurance law of 1883 covered blue-collar workers in selected industries, craftspeople and other selected professionals.6 It is estimated that this law brought health insurance coverage up from 5 to 10 per cent of the total population.
Bärnighausen, Till; Sauerborn, Rainer (May 2002). "One hundred and eighteen years of the German health insurance system: are there any lessons for middle- and low income countries?" (PDF). Social Science & Medicine. 54 (10): 1559–1587. doi:10.1016/S0277-9536(01)00137-X. PMID 12061488. Retrieved March 10, 2013.As Germany has the world’s oldest SHI [social health insurance] system, it naturally lends itself to historical analyses
- "Duden - Krankenkasse - Rechtschreibung, Bedeutung, Definition, Synonyme". duden.de.
- The use of the term "Krankenkasse" for both public and private health insurances is so widespread that Duden doesn't even label this usage as colloquial.
- "The Case for Universal Health Care in the United States". Cthealth.server101.com. Retrieved 2011-08-06.
- "German Health Care System – an Overview - Germany Health Insurance System". germanyhis.com.
- DiPiero, Albert (2004). "Universal Problems & Universal Healthcare: 6 COUNTRIES — 6 SYSTEMS" (PDF). Archived from the original (PDF) on 21 February 2006.
- A. J. W. Goldschmidt: Der 'Markt' Gesundheitswesen. In: M. Beck, A. J. W. Goldschmidt, A. Greulich, M. Kalbitzer, R. Schmidt, G. Thiele (Hrsg.): Management Handbuch DRGs, Hüthig / Economica, Heidelberg, 1. Auflage 2003 (ISBN 3-87081-300-8): S. C3720/1-24, with 3 revisions / additional deliveries until 2012
- World Health Organization Statistical Information System: Core Health Indicators
- Germany country profile. Library of Congress Federal Research Division (December 2005). This article incorporates text from this source, which is in the public domain.
- "Outcomes in EHCI 2015" (PDF). Health Consumer Powerhouse. 26 January 2016. Archived from the original (PDF) on 2017-06-06. Retrieved 27 January 2016.
- "Überschüsse bei den Krankenkassen – wohin mit dem Geld?". Medscape (in German). Retrieved 2019-03-17.
- Clarke, Emily. "Health Care Systems: Germany" (PDF). Civitas. Archived from the original (PDF) on 2013-10-05. Retrieved 25 September 2013.
- "History of German Health Care System". Photius.com. Retrieved November 14, 2011.
- "Gesetzliche Krankenversicherungen in Vergleich". Archived from the original on 2014-06-01. Retrieved 2009-01-25.
- Kirkman-Liff BL (1990). "Physician Payment and Cost-Containment Strategies in West Germany: Suggestions for Medicare Reform". Journal of Health Care Politics, Policy and Law (Duke University). 15 (1): 69–99. doi:10.1215/03616878-15-1-69. PMID 2108202.
- Henke KD (May 2007). "[External and internal financing in health care]". Med. Klin. (Munich) (in German). 102 (5): 366–72. doi:10.1007/s00063-007-1045-0. PMID 17497087.
- "Germany: Health reform triggers sharp drop in number of hospitals". Allianz. 25 July 2005. Retrieved November 14, 2011.
- "Average Length of Hospital Stay, by Diagnostic Category --- United States, 2003". Centers for Disease Control and Prevention. Retrieved November 14, 2011.
- Borger C, Smith S, Truffer C, et al. (2006). "Health spending projections through 2015: changes on the horizon". Health Aff (Millwood). 25 (2): w61–73. doi:10.1377/hlthaff.25.w61. PMID 16495287.
- E. REINHARDT, UWE. "A German Import That Could Help U.S. Health Reform". The New York Times. Retrieved 25 May 2013.
Germany’s joint committee was established in 2004 and authorized to make binding regulations growing out of health reform bills passed by lawmakers, along with routine coverage decisions. The ministry of health reserves the right to review the regulations for final approval or modification. The joint committee has a permanent staff and an independent chairman.
- "An education handbook about the federal joint committee and its tasks, published by the federal medical association in germany" (PDF). website of the German federal medical association. 2009.
- Busse, Reinhard; Blümel, Miriam; Knieps, Franz; Bärnighausen, Till (August 2017). "Statutory health insurance in Germany: a health system shaped by 135 years of solidarity, self-governance, and competition". The Lancet. 390 (10097): 882–897. doi:10.1016/S0140-6736(17)31280-1. ISSN 0140-6736. PMID 28684025.
- "Private or public? An introduction to German health insurance". allaboutberlin.com. Retrieved 2019-02-06.
- David Squires; Robin Osborn; Sarah Thomson; Miraya Jun (November 14, 2013). International Profiles of Health Care Systems, 2013 (PDF) (Report).
- Schmitt, Thomas (21 May 2012). "Wie Privatpatienten in die Krankenkasse schlüpfen" (in German). Handelsblatt.
- SOEP – Sozio-oekonomische Panel 2006: Art der Krankenversicherung
- "Nicht verfügbar". pflegeversicherung-test.de.
- "Nicht verfügbar". pflegeversicherung-test.de.
- "Vorsicht Pflege-Bahr: Stiftung Warentest rät von staatlich geförderten Pflege-Tarifen ab". 16 April 2013 – via FAZ.NET.
- National Association of Statutory Health Insurance Funds: List of German Public Health Insurance Companies Archived 7 June 2015 at the Wayback Machine
- Mannheim Institute of Public Health (MIPH), Heidelberg University: Understanding the German Health Care System
- "Liste aller Krankenkassen". gesetzlicheKrankenkassen.de (in German). Retrieved 2019-09-05.
- J. Kartte, K. Neumann: Der zweite Gesundheitsmarkt. Die Kunden verstehen, Geschäftschancen nutzen, o.O.: Roland Berger Strategy Consultants, München, 2007
- Pfeiffer D, Spitzenverband der Gesetzlichen Krankenkassen GKV →Mitteilung im Nachrichtendienst dapd vom 4. February 2012
- "Plan your treatment". https://www.helios-gesundheit.de/ (in German). Retrieved 2019-03-19. External link in
|website=(help) - heidelberg-university-hospital.com https://www.heidelberg-university-hospital.com/treatment-inquiry-appointment/. Retrieved 2019-03-19. Missing or empty
|title=(help) - A. J. W. Goldschmidt: Leading the Global Game - M&A between Competitiveness and Conflicts. Speech as „guest speaker“ with round table-discussion „health economy and logistics“, 9th Symposium of Organisationsforum Wirtschaftskongress e.V. in the University of Applied Science Cologne on March, 8th 2002
- A. J. W. Goldschmidt: Paragraph „Unternehmensbedeutung“ in: Krankenhausmanagement mit Zukunft?. In: A. J. W. Goldschmidt, J. Hilbert (Hrsg.): Krankenhausmanagement mit Zukunft - Orientierungswissen und Anregungen von Experten. kma Medien in Georg Thieme Verlag KG, Stuttgart, 2011, (ISBN 978-3-13- 161231-1): p. 4.
- Josef Hilbert
- E. Dahlbeck, J. Hilbert: Beschäftigungstrends in der Gesundheitswirtschaft im regionalen Vergleich. Internet-Dokument. Gelsenkirchen: Inst. Arbeit und Technik. Forschung Aktuell, Nr. 06/2008 → http://www.iat.eu/forschung-aktuell/2008/fa2008-06.pdf
- A. J. W. Goldschmidt, J. Hilbert: Von der Last zur Chance – Der Paradigmenwechsel vom Gesundheitswesen zur Gesundheitswirtschaft. In: A. J. W. Goldschmidt, J. Hilbert (Hrsg.): Gesundheitswirtschaft in Deutschland. Die Zukunftsbranche. Band 1 der Schriftenreihe: Gesundheitswirtschaft und Management. kma-Reader - Die Bibliothek für Manager. Wikom-Verlag (Thieme), Wegscheid, 2009 (ISBN 978-3-9812646-0-9): p. 20-40
- Statistisches Bundesamt: Beschäftigung in der Gesundheitswirtschaft steigt weiter an. Pressemitteilung Nr. 490, Berlin, 17.12.2008
- Statistisches Bundesamt Deutschland, Wiesbaden, 2012
- B. Häusler, A. Höer, E. Hempel: Arzneimittel-Atlas 2012. Springer, Berlin u. a. 2012 (ISBN 978-3-642-32586-1) Archived 2013-01-01 at the Wayback Machine
- "How Germany is reining in health care costs: An interview with Franz Knieps | McKinsey". mckinsey.com. Retrieved 2019-06-28.
- Hossein, Zare; Gerard, Anderson (2013-09-01). "Trends in cost sharing among selected high income countries—2000–2010". Health Policy. Health System Performance Comparison: New Directions in Research and Policy. 112 (1): 35–44. doi:10.1016/j.healthpol.2013.05.020. ISSN 0168-8510. PMID 23809913.
- Office of health Economics. "International Comparison of Medicines Usage: Quantitative Analysis" (PDF). Association of the British Pharmaceutical Industry. Archived from the original (PDF) on 2015-11-11. Retrieved 2 July 2015.
- Ballas, Dimitris; Dorling, Danny; Hennig, Benjamin (2017). The Human Atlas of Europe. Bristol: Policy Press. p. 79. ISBN 9781447313540.
- Length of hospital stay, Germany group-economics.allianz.com, undated
- Length of hospital stay, U.S. MMWR, CDC
- Borger C, Smith S, Truffer C, et al. (2006). "Health spending projections through 2015: changes on the horizon". Health Aff (Millwood). 25 (2): w61–73. doi:10.1377/hlthaff.25.w61. PMID 16495287.
- "NHS Health Check: How Germany's healthcare system works". BBC News. 9 February 2017. Retrieved 10 February 2017.
- Siciliani, S., & Hurst, J. (2003). Explaining Waiting Times Variations for Elective Surgery across OECD Countries. OECD Health Working Papers, 7, 8, 33-34, 70. https://dx.doi.org/10.1787/40674618616
- The Commonwealth Fund. (2010). Commonwealth Fund 2010 Health Policy Survey in 11 Countries (pp. 19-20). New York, NY: Author. Accessed from http://www.commonwealthfund.org/~/media/files/publications/chartbook/2010/pdf_2010_ihp_survey_chartpack_full_12022010.pdf
- Kassenärztliche Bundesvereinigung. (2016). Health data: Die Wartezeit ist für die meisten kurz The wait is short for most. Retrieved from Google Translate
- "Organization for Economic Cooperation and Development - Health at a Glance 2011: OECD Indicators". 2011.
- Busse R., & Blümel, M. (2014). Germany: health system review. Health Systems in Transition, 16(2), 142-148. Available from http://www.euro.who.int/__data/assets/pdf_file/0008/255932/HiT-Germany.pdf?ua=
Germany articles | ||||||
|---|---|---|---|---|---|---|
| History |
|  | ||||
| Geography |
| |||||
| Politics |
| |||||
| Economy |
| |||||
| Society |
| |||||
| ||||||